Urinalysis is an important diagnostic tool in veterinary practice. It is indicated for any patient that presents with polyuria or urinary tract signs, but also a necessary test to perform in conjunction with serum biochemistry.
Urine sediment exams on Christmas day.
Why do some clinicians fail to perform urinalyses even when they are indicated?
Reasons include:
clinicians not seeing the importance of obtaining a urine sample
the difficulty of obtaining a sample in some situations (the patient may not want to void)
no access to an ultrasound for a guided cystocentesis
patients not urinating upon bladder expression
Make it a priority
However, it is important clinicians make obtaining a urine sample a priority. Where possible, a sterile sample of urine using ultrasound-guided cystocentesis is recommended, especially when there is a possibility the urine may be sent to an external lab for culture and sensitivity.
For example, we’ve all been in situations were you start a patient on IV fluids only to find an azotemia on blood tests. Now you can’t determine whether it’s a pre-renal or renal cause, as you don’t have a pre-IV fluid urine sample.
Also it would be best to avoid the situation where you have run all other tests available on an ill patient only to find the answer lay in that urinalysis you did not collect earlier.
You’re stuck in the clinic in the middle of the night with a dog that is dying – it’s bleeding into its abdomen and needs blood, but the bag in the fridge is expired.
You’ve heard it’s possible to collect the blood out of the abdomen and safely give it to the patient, but you’re not sure how and don’t have time to google. How do you actually do it?
It’s easier than you think. Depending on what equipment you have available in the clinic, here are two practical ways of administering an autotransfusion.
Collection
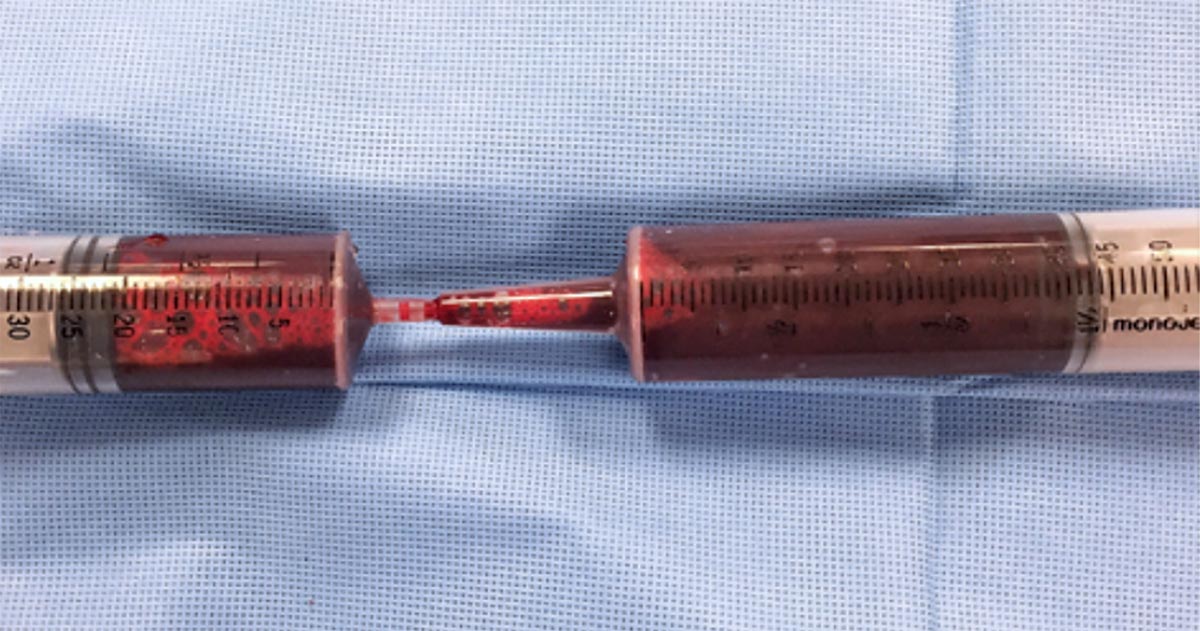
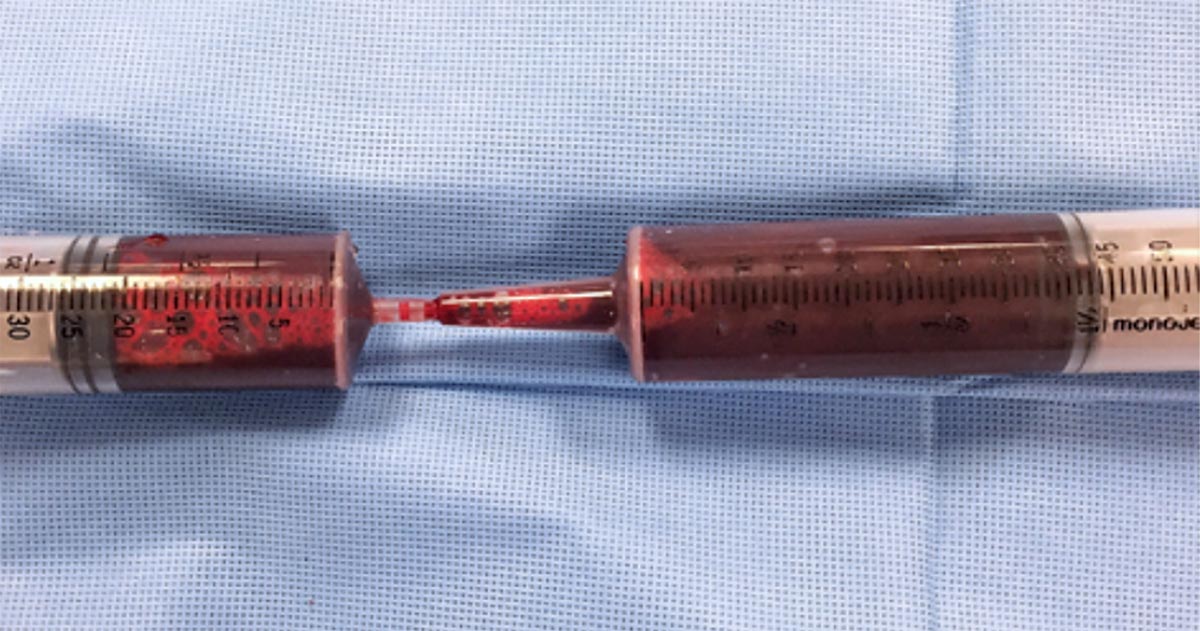
Blood can be collected from the abdomen or thorax during exploratory surgery, simply by sucking it up with a 60ml syringe.
Time is usually of the essence in these cases, so a handy tip is to use 60ml catheter tip syringes to aspirate the blood, then get someone to transfer the blood into a standard Luer-tipped syringe by shoving the smaller tip into the catheter tip. Like this:
Besides the faster collection time, the bigger aperture of the catheter tip syringe will also reduce negative pressure during collection and, therefore, the chances of haemolysis.
If you are not going into surgery, you can collect the blood percutaneously – using a butterfly needle or catheter – as you would drain any body cavity fluid.
You shouldn’t need to add any anticoagulants to your syringes, as fibrinolysis has already occurred – meaning the blood shouldn’t clot in your syringe.
Administration
Whichever method you use, it’s crucial the blood is administered through a blood filter.
Method one
The most straightforward way is to simply inject the blood back into the patient using the Luer-tipped syringe through a filter. For this technique, you will need a filter that can connect to a syringe.
Method two
If you only have a blood filter as part of a blood giving set, you could use a two-way stopcock valve to get your collected blood into a sterile bag – like an empty IV fluids bag, or a dedicated blood collection bag – and then run the blood through your blood giving set with the built-in filter, as you would for a normal transfusion.
This is a bit more fiddly, so adding a few little blood filters to your emergency equipment could be well worth your time.
When you shouldn’t do it
Autotransfusions are most useful in cases of bleeding due to clotting deficiencies where the clotting problem is already being addressed, but a need for red blood cells still exists; and for cases of traumatic or postoperative bleeding.
It is contraindicated if contamination with urine, faeces, bile or bacteria – in case of septic peritonitis – is likely; or in cases of neoplasia in the body cavity where an autotransfusion has the potential to seed neoplastic cells to the rest of the body.
Thrombocytopenia is a condition characterised by a decrease in platelet numbers, which is often caused by increased destruction of platelets or a decrease in production.
Thrombocytopenia can manifest in many ways – the signs can be subtle and easily missed, such as small petechiae on gums, or quite obvious signs, such as large areas of ecchymotic haemorrhage on the skin.
Ecchymotic haemorrhages are often attributed to disorders of secondary haemostasis, such as rodenticide intoxication, but it can also occur with thrombocytopenia depending on the severity and chronicity.
Other common clinical signs include:
epistaxis
blood in stools, urine or vomit
pale mucus membranes
lethargy
weakness
Therefore, the first step to managing a patient with a severe thrombocytopenic episode that has resulted in significant blood loss is to manage shock, if present, with IV fluids, then administer a red blood cell transfusion.
Patient handling
Careful patient handling is critical as these patients can bleed easily, leading to blown veins, large bruises that contribute to the development of anaemia and significant patient discomfort. Beyond initial patient stabilisation, the next step is to determine the underlying cause.
Diagnosing thrombocytopenia is relatively straightforward with the demonstration of low platelet counts. Generally, bleeding does not occur until the platelet count drop below 40,000 thousands per cubic milliliter (k/uL). This can be determined by either a haematology machine or manually via blood smear analysis.
When assessing blood smears, the general rule is one platelet per high-powered field on the monolayer is equal to 15,000k/uL. With either method, you must assess for platelet clumping on a blood smear as this can artefactually drop platelet numbers, leading to a false diagnosis.
The diagnostic pathway should not stop there. It needs to continue to determine the underlying cause.
The most common cause of thrombocytopenia is immune-mediated destruction. This can be either a primary (diagnosis of exclusion) or secondary cause (such as Rickettsia infection, and drugs such as sulphonamides, toxins and neoplasia). Other less common causes include:
splenomegaly, which can lead to platelet sequestration
disseminated intravascular coagulation and acute blood loss, leading to platelet consumption
bone marrow disease, which results in reduced platelet production
Signalment and history will refine such a diagnosis, as certain breeds are more prone to developing thrombocytopenia than others – for example, grey collies due to a defect in haematopoietic stem cells, and whippets and greyhounds, which traditionally have a lower platelet count than other breeds.
The generally diagnostic pathway continues to include haematology and biochemistry, thoracic radiographs, abdominal ultrasound and depending regional prevalence testing for infectious organisms with PCR and ELISA assays.
Next week I will cover the management principles of the thrombocytopenic patient.
A lot of information is available regarding different antibiotics and, for the newest generation of vets, the pressure to use them correctly and responsibly is greater than ever.
One of main challenges when you start clinical practice is knowing the most appropriate antibiotic for common presenting conditions.
Below is a rough guide for antibiotic selection according to body system. However, make sure you stick to the following rules:
Limit antibiotic use to animals that actually require them – resist the urge to dispense them due to pressure from owners or when you feel there is nothing else to turn to.
What is the likely type of bacteria you are aiming to target (such as anaerobes, Gram-positives and Gram-negatives)? Collect samples from lesions/discharge or effusions/blood and urine, and see if there is evidence of bacteria under the microscope.
Use the most narrow spectrum antibiotic as possible.
Perform a culture and sensitivity whenever possible – especiallyif a case does not respond to your first line antibiotic.
Avoid using fluoroquinolones, third and fourth generation cephalosporins and amikacin without evidence of resistance from culture and sensitivity results.
Use an appropriate dosage regime and make sure the owners have the capacity to administer them accordingly.
Skin
Try topical chlorhexidine alone if surface pyoderma
Clindamycin
Cephalexin
Amoxicillin-clavulanic acid
Upper respiratory tract
Doxycycline
Amoxicillin-clavulanic acid
Lower respiratory tract
Amoxicillin-clavulanic acid
Ampicillin
GI tract
Metronidazole (research questions the use of antibiotics for diarrhoea cases)
Tylosin (chronic diarrhoea)
Urogenital tract
Remember that cystitis in cats is often stress-related rather than due to infection
Last week we gave some hints and tips about how to perform a thoracocentesis. This week we look at what to do with the sample you collected and where to go to next.
Looking at the sample is not enough, there are several things you need to do to make sure you are getting the most information from the collected sample. This includes:
Fluid cell counts
Total protein assessment
Packed cell volume
Glucose
Lactate (if it is an exudate)
In-house cytology
Collect a sample for culture and sensitivity, and also external cytology assessment
With this information you can narrow down your list of differentials; often enough it can give you a diagnosis.
Here is the list I use. Note, it is not exhaustive and assumes you have taken three-view thoracic radiographs as part of the initial diagnosis.
Transudate
Haemorrhagic effusion.
Clear appearance – characterised by low protein and low cellularity
Transudates are caused by reduced oncotic pressure
Total nucleated cell counts = <0.5x10e9/L
Total protein = <25g/L
Differentials to consider
Liver disease
Protein-losing nephropathy
Protein-losing enteropathy
Additional diagnostics
Cytology and culture of fluid
Haematology and biochemistry
+/- dynamic liver testing
Urinalysis, urine protein/creatinine ratio, culture and sensitivity
Modified transudate
Yellow/serosanguinous/cloudy appearance
Caused by increased hydrostatic pressure leading to passive leakage of proteins and fluid into the pleural space
Total nucleated cell counts = 3.5-5x10e9/L
Total protein = variable, ~25-50g/L
Differentials to consider
Increased capillary hydrostatic pressure and pericardial disease
Diaphragmatic hernia
Neoplasia
Lymphatic obstruction, such as neoplasia, diaphragmatic hernia and abscess
Increased permeability of vessels (blood and lymphatics), such as FIP
Additional diagnostics
Cytology and culture of fluid
Haematology and biochemistry
Cardiac auscultation and ultrasound
+/- CT
Exudate
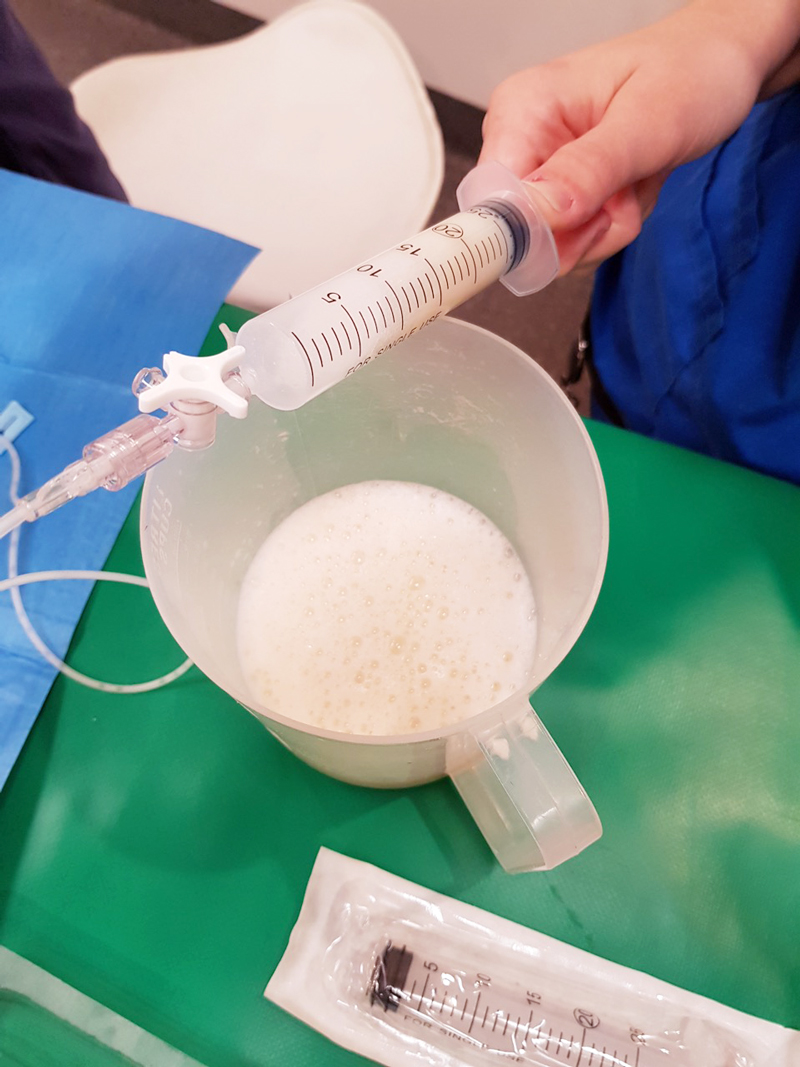
Turbid appearance – Very proteinaceous liquid, froths when shaken
Fluid is a mix of plasma and inflammatory mediators, and is caused by either septic or aseptic inflammation
Total nucleated cell counts = >3.0x10e9/L
Total protein = >30g/L
Aseptic exudate
Non-degenerate neutrophils and activated mesothelial cells predominate
Non-infectious cause
Differentials
Inflammation: FIP (can have high globulins), liver disease, lung torsion and hernia
Neoplasia
Additional diagnostics
Haematology and biochemistry
Cytology and culture of fluid
+/- ultrasound/CT
Further testing for FIP
Septic exudate
Degenerate neutrophils predominate: nuclear swelling and pale staining
Intracellular or extracelluar microorganisms
Culture and sensitivity: aerobic and anaerobic
Pleural fluid [glucose] < serum [glucose]
Pleural fluid [lactate] > serum [lactate]
Differentials to consider
Ruptured abscess
Foreign body inhalation or penetrating injury
Fungal infection
Additional diagnostics
Haematology and biochemistry
Cytology and culture of fluid
+/- ultrasound/CT
Chyle
Chyle.
Opaque (milky) to pink.
Differentials to consider
Rupture or obstruction of lymphatic flow
Neoplasia, traumatic and idiopathic
Secondary to heart failure (especially in cats)
Pseudochyle (usually formed by lymphoma)
Additional diagnostics
CBC and biochemistry
Cytology and culture of fluid
Fluid [TAG] > serum
Large number of lymphocytes and other inflammatory cells
+/- ultrasound/CT
Haemorrhage
Red blood cells
True haemorrhagic; for example, not iatrogenic: should not see platelets or erythophagocytosis on smears and sample should not clot
Time frame
Assess history
Compare fluid PCV/total protein (TP) to peripheral PCV/TP:
<1% – non-significant
1% to 20% – neoplasia, trauma, pneumonia
>50% – haemothorax
Other tips:
If PCV/TP is similar = recent bleed, if PCV is low and TP normal = chronic
If PCV is increasing or is higher than peripheral then active bleeding
Presence of erythrophagocytosis = chronic
Differentials to Consider
Trauma
Neoplasia
Coagulopathies
Ruptured granuloma
Diagnostics
Activated clotting time, activated partial thromboplastin time, prothrombin time, blood smear and other coagulation tests, see “coagulopathy”
Blood smear
CBC and biochemistry
+/- ultrasound/CT
Good luck with your next thoracocentesis. I hope this information was useful.
The causes of hyponatraemia can be divided into three major categories, based on serum osmolality. This is further divided based on the patient’s volume status (Table 1).
Most patients we see in clinic fall into the hypovolaemic category, except patients with diabetes mellitus.
Table 1. Causes of hyponatraemia based on osmolality and volume status (from Guillaumin and DiBartola, 2017).
Hypo-osmolar
Hyperosmolar
Normo-osmolar
Hypovolaemic
Normovolaemic
Hypervolaemic
Gastrointestinal fluid loss
Third-space fluid losses
Shock
Hypoadrenocorticism (Addison’s disease)
Renal insufficiency
Excessive diuretic administration
Salt-losing nephropathy
Cerebral salt wasting syndrome
Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
Hypotonic fluid administration
Hypothyroidism
Glucocorticoid insufficiency
Psychogenic polydipsia
Reset osmostat (SIADH type B)
Congestive heart failure
Acute or chronic renal failure
Nephrotic syndrome
Hepatic cirrhosis
Accidental ingestion or injection of water (water intoxication)
Hyperglycaemia
Mannitol
Severe azotaemia
Hyperlipidaemia
Hyperproteinaemia
Common causes
In dogs, the three most common causes of hyponatraemia are:
gastrointestinal (GI) fluid loss
third-space fluid loss
fluid shift from intracellular fluid to extracellular fluid (ECF) as a result of hyperglycaemia
In cats, the three most common causes of hyponatraemia are:
urologic diseases
GI fluid loss
third-space fluid losses
In most patients, more than one pathophysiologic factor is likely to be contributing to the hyponatraemia.
Circulating volume
Hypovolaemic patients – those with, for example, GI losses, hypoadrenocorticism, renal losses and haemorrhagic shock – have a reduced effective circulating volume. ECF contraction triggers antidiuretic hormone (ADH) secretion, which leads to increases in free water absorption and thirst, and results in dilution of the serum sodium concentration. Aldosterone secretion is reduced in hypoadrenocorticism, so an overall reduction in sodium reabsorption compounds the problem.
Hypervolaemic patients are those with an increased fluid retention state, such as:
Congestive heart failure patients have a reduced cardiac output and, therefore, a decreased effective circulating volume, despite the presence of the extra fluid status. Renin-angiotensin activation leads to release of ADH and aldosterone, resulting in sodium and free water reabsorption, and increased thirst. Both lead to an excess of free water retention.
Advanced hepatic (cirrhosis) or renal failure (nephrotic syndrome) both result in hypoalbuminaemia, leading to fluid shifting into the interstitial space and third space, reducing effective circulating volumes. This leads to activation of ADH to increase free water reabsorption, to restore the circulating volume in the face of existing hypervolaemia and hyponatraemia.
Diabetic patients
Moderate to severe hyperglycaemic diabetic patients can be either hyperosmolar or normo-osmolar, depending on the serum blood glucose concentration. Hyponatraemia occurs when water shifts from the intracellular fluid to the ECF down the osmotic gradient, diluting the serum sodium content.
Despite this osmotic shift, not all diabetic patients develop hyponatraemia. Glucosuria also causes also causes a renal osmotic shift, sometimes resulting in urine water loss in excess to sodium. This offsets the hyponatraemia – in some cases, hypernatraemia results.
Treatment
Treatment of hyponatraemia hinges on how quickly it developed and the volume status of the patient. The rule of thumb is to correct hyponatraemia slowly – not exceeding 0.5meq/L/hr – especially in chronic cases, or cases where the duration of hyponatraemia is unknown. Keeping to this rate is paramount until serum sodium concentration reaches 130meq/L.
In acute patients with severe clinical signs, such as seizures, some clinicians may choose to use a higher rate of 1meq/L/hr to 2meq/L/hr until clinical signs resolved.
It should be emphasised, once again, this rate should never be used in chronic patients, patients with an unknown duration of hyponatraemia, or where frequent serum sodium concentration cannot be monitored. The rapid correction of hyponatraemia can lead to osmotic demyelination syndrome (myelinolysis).
Its effect will not be apparent until three or four days after therapy, and can result in neurological abnormalities such as:
weakness
ataxia
dysphagia
paresis
coma
For that reason, frequent electrolyte measurements are required, starting hourly then once a suitable rate of increase has been established and less frequently thereafter.
Part 3 will look at how to correct patients with hyponatraemia.
Reference
Guillaumin J and DiBartola SP (2017). A quick reference on hyponatremia, Veterinary Clinics of North America: Small Animal Practice47(2): 213-217.
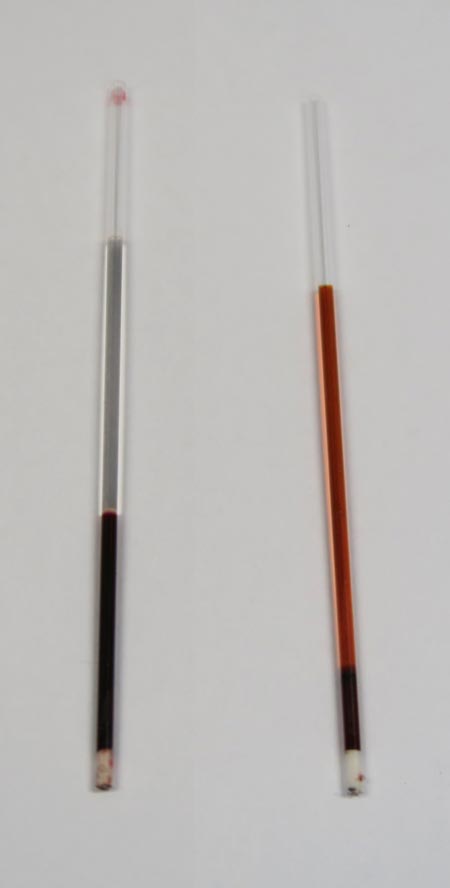
When interpreting the often misinterpreted and underused PCV and total solids test, it is important to take note of the serum colour as this may give clues into the diagnosis.
Normal serum colour (left) compared to a patient with immune-mediated haemolytic anaemia. The serum is haemolysed and anaemia is present.
The most common abnormalities seen in clinic are icteric, haemolysed and lipaemic serum.
Clear serum can also be of importance – especially when you interpret it with blood counts and urine colour.
Haemolysis
The most common abnormality of serum colour changes is haemolysis. In my experience, the most common cause is suboptimal collection technique. To confirm this, simply collect another sample and repeat.
If it is repeatable, and concurrent anaemia or pigmenturia is present, it warrants further investigation.
Intravascular haemolysis can be caused by:
immune-mediated haemolytic anaemia
blood transfusion reactions
infectious diseases such as Mycoplasma haemofelis, Babesia canis, Ehrlichia canis, FeLV and others
Heinz bodies from the ingestion of heavy metal, onions or paracetamol
hypophosphataemia
macroangiopathic disease (neoplasia, for example)
envenomation – typically, snake bites
Testing issues
Haemolysis can also affect other laboratory testing. It can lead to an artefactual increase in glucose, phosphorus, bilirubin, total protein, fructosamine and triglycerides, and a decrease in sodium (pseudohyponatraemia), cholesterol, calcium, potassium and albumin.
Extravascular haemolysis often does not cause haemolysed serum as it is generally slower and the body is able to clear the haemoglobin before it can lead to discolouration of the serum.
Postoperatively, gastric dilatation-volvulus (GDV) patients remain in our intensive care unit for at least two to three days.
Monitoring includes standard general physical examination parameters, invasive arterial blood pressures, ECG, urine output via urinary catheter and pain scoring.
I repeat PCV/total protein, lactate, blood gas and activated clotting times (ACT) immediately postoperatively and then every 8-12 hours, depending on abnormalities and patient progress.
Patient recovering in the pet intensive care unit. As well as standard monitoring parameters, GDV patients have constant ECG, arterial blood pressure and urine output monitoring to enable the early detection and correction of abnormalities.
I always repeat these blood tests postoperatively, as IV fluids given during the resuscitation and intraoperative period often cause derangements. I use the results to guide my fluid therapy, but also take it with a grain of salt.
IV fluids
I generally continue a balanced and buffered crystalloid. The rate depends on blood pressures, urine output and assessment of general physical examination parameters for perfusion and hydration, but I try to avoid fluid overload and reduce the IV fluids postoperatively as soon as possible.
Coagulopathy
Prolonged clotting times are frequently seen as a result of consumption in a dog with GDV. However, one should note it can also occur as the result of haemodilution.
As the underlying disease process has been corrected, and haemostasis achieved during surgery, I usually monitor ACTs, but may not necessarily treat with blood products as prolonged ACTs do not always translate to clinical bleeding. Unless clinical evidence of bleeding exists, I generally hold off treatment and monitor.
Hypoproteinaemia
Low total protein is also common. This is generally due to haemodilution from fluid resuscitation. However, a low total protein does not mean oedema will develop, or that it requires management. I generally track the protein levels, use conservative fluid therapy and try to correct it by instituting enteral nutrition as soon as possible.
Electrolyte imbalances
Hypokalaemia is a common complication of fluid therapy. This can be rectified with potassium supplementation in the IV fluids.
Hyperlactataemia
If present post-surgery, this is usually corrected with a fluid bolus. However, I always assess for other things that may affect oxygen delivery to the tissues, such as poor cardiac output (arrthymias), hypoxaemia (respiratory disease) and anaemia (from surgical blood loss).
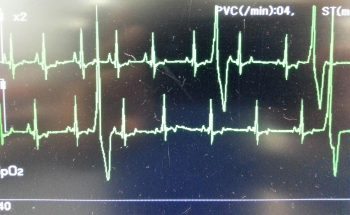
Arrhythmias
Ventricular arrhythmias are common post-surgery. Accelerated idioventricular rhythms are the most common cause, especially if a splenectomy was performed.
Ventricular premature contractions are common postoperative arrhythmia.
Before reaching for anti-arrythmia medications, first check and correct:
electrolyte abnormalities
hypoxaemia
pain control
hypovolaemia or hypotension
If they are still present, despite correction of the above, consider treating the rhythm if:
multifocal beats (ventricular premature contractions of various sizes)
overall rate greater than 190 beats per minute
R-on-T phenomenon
low blood pressure during a run of ventricular premature contractions
I start with a bolus 2mg/kg lidocaine IV and start a constant-rate infusion of 50ug/kg/min to 75ug/kg/min.
Anaemia
It is common to have a mild anaemia post-surgery, due to a combination of blood loss and haemodilution. In the absence of transfusion triggers – such as increased heart rate, increased respiratory rate or hyperlactataemia – it does not require treatment.
Vomiting
Anti-emetics are the first line of medication. Non-prokinetic anti-emetics, such as maropitant and ondansetron, can be used immediately; otherwise, after 12 hours, metoclopramide can also be used postoperatively. If the patient remains nauseous despite these medications, the placement of a nasogastric tube can ease nausea by removing static gastric fluid.
Excessive pain relief may also contribute to the nauseous state.
Pain relief
I mostly rely on potent-pure opioid agonists, such as fentanyl constant-rate infusions and patches. This is generally sufficient for most patients. Ketamine is occasionally used.
Some drugs listed in this article are used under the cascade.
Christmas can be a busy time for vet clinics, so here is a list of common intoxications and conditions to keep an eye out on during the festive period.
Chocolate
Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.
I always perform emesis in patients that have ingested chocolate, even hours after ingestion as often large amounts can reside in the stomach.
Remember that cardiac arrhythmias can also occur in clinically normal looking patients, so perform an ECG.
The toxic components can be reabsorbed through the bladder wall; therefore, urinary catheterisation is a part of management of this intoxication.
Onions
Onions used in roasts and on BBQ’s can cause Heinz body formation, haemolytic anaemias and pigmenturia.
This is not a common intoxication, but should be considered in anaemia patients and those with discoloured urine.
Raisins
Commonly used in Christmas cakes and puddings. They can cause acute kidney failure, the exact mechanism of action is unknown, and there does not appear to be a dose-dependent relationship.
It should always be a differential for azotemic patients this time of year.
IV fluid induced diuresis for 48 hours is the safest way to manage raisin exposure.
Mistletoe
The berries can be fatal, even if only a couple are ingested.
Ethylene glycol
In colder climates, ethylene glycol can be a very common toxicity.
This sweet liquid is very attractive to pets and can cause acute renal failure, with the first signs being acute onset ataxia.
Macadamia nuts
Macadamia nuts are common in some parts of the world. They result in joint pain in the hocks and carpus leading to weakness and ataxia.
Often confused with trauma and soft tissue injuries. Hyperextension of the hocks and sometimes flexion of the carpus are the clinical features.
Xylitol
Xylitol is a sugar-free product used in lollies and baking.
In dogs, it triggers endogenous insulin to be released and a subsequent hypoglycemia develops. It can also cause hepatic failure.
As a general rule, I approach all intoxications as if they could be fatal as it is rare to know exactly how much of the toxic agent they have been exposed to. I consider if a patient I am treating for intoxication never develops clinical signs and wonder whether it was going to or not is the best outcome.
Strings
Look under the tongue.
Linear foreign bodies can be difficult to diagnose. Some features on abdominal radiographs to look out for include abnormal bunching of the small intestines, and “c” and “comma” shaped gas patterns.
Christmas meals
Gastroenteritis is the most common presenting condition over the Christmas period, with dietary change and indiscretion often being the culprit.
Bones can lead to obstructions from oral cavity to the intestines and can also cause constipation.
Leftover meat trimmings, often fat laden, are a common cause of pancreatitis.
BBQ skewers
In some parts of the world (Australia especially) BBQs are common around Christmas time.
BBQ skewers can cause gastrointestinal tract perforation and septic peritonitis.
Because they are not radiopaque they are often difficult to diagnose.
Obstructive feline lower urinary tract disease (FLUTD) is a common presentation in both general practice and emergency settings.
Every clinician has his or her own approach to treating and managing a cat with obstructive FLUTD signs. Working in an emergency setting, once I have confirmed an obstructed bladder via palpation, I focus on trying to relieve the obstruction as quickly as possible.
The first step is obtaining consent from the client to administer pain relief (an opioid IV or IM), place an IV catheter, collect blood for biochemistry, electrolyte and blood gas analysis, and temporarily relieve the obstruction.
At our hospital, we achieve temporary relief of the obstruction generally within 15 minutes of patient arrival.
Process
Obstructive feline lower urinary tract disease is a common presentation in general practice.
We do this in three steps:
Assess the tip of the penis, occasionally a crystal/mucus plug is all that is blocking the penis.
If this is not the case, I pass a pre-lubricated 22g IV catheter tip (without the stylet) into the penis with a 10ml syringe, containing 0.9% NaCl, connected for hydropropulsion. In the vast majority of cases, this helps to dislodge the urethral blockage enough to enable some urine to pass (urination suggests active urination by the cat).
Once urine is flowing, I pass a 12cm or 14cm rigid catheter, tape it to the tail and leave it in place to allow constant drainage.
If the 22g IV catheter does not relieve the obstruction, I would use a rigid catheter and progressively advance it up the urethra while hydropropulsing with the saline the entire time. Once unblocked, then I will tape it to the tail as aforementioned.
Quick Tip: Once you have the catheter in the tip of the penis, pull the prepuce straight out to straighten the penis and thus the penile urethra. Otherwise, the bend in the penile urethra may hinder the passage of the catheter.
Benefits
The benefits I see of placing a temporary urinary catheter include:
immediate relief to the patient and reduces their stress levels
provides a sample for urinalysis
allows you time to run through the diagnostic and treatment plan in more detail with clients
buys you time to stabilise the patient for their anaesthetic later to place a closed system indwelling urinary catheter and then bladder lavage
Quite often, your patient would present unwell enough that you should have no issues (resistance to) passing this temporary urinary catheter, provided you have given pain relief on presentation.
In fractious patients, I usually forgo the temporary catheter and focus on stabilising the patient. The aim is to have them stable as soon as possible for sedation or a general anaesthesia to place a longer indwelling urinary catheter.











 Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.
Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.
