It has been proven that you learn better and recall more information when you are expected to teach someone, compared to when you are expecting to be examined on it.
So, how can you take advantage of this, and what are the benefits?
The benefit of sharing knowledge is twofold – you benefit, but so do others. There is no point holding on to what you know if your colleagues, community and patients can benefit from it.
Teaching not only benefits others, but also makes sure you understand what you are talking about.
The questions you get asked highlight the common aspects you should know and highlight areas you need to learn in more depth.
Practical application
I use this by thinking of something I want to know more about, or be better at – and I pre-organise having to teach it to others.
I recently used this with ECG interpretation at our hospital, which we are competent at, but not great.
We were limited as we were all teaching each other little bits and pieces here and there, but no one was really 100% clear about the topic. So I decided it had been on my bucket list for long enough and booked a tutorial one month in advance. I then scheduled in reading and time to prepare, then deliver, a presentation.
As I was learning it, I made sure I knew it well enough so I could pass on that knowledge and train others to do the same. I have now delivered the presentation twice.
I guarantee you, this is a very effective method of learning and has benefited not only myself, but the whole team.
Treatment of ionised hypocalcaemia (iHCa) is reserved for patients with supportive clinical signs, then divided into acute and chronic management.
Since the most common cases of clinical hypocalcaemia in canine and feline patients are acute to peracute cases, this blog will focus on the acute treatment and management of hypocalcaemia.
Clinical signs
The severity of clinical signs of iHCa is proportional to the magnitude, as well as the rate of decline in ionised calcium (iCa) concentration.
The normal reference range for iCa is 1.2mmol/L to 1.5mmol/L in dogs and 1.1mmol/L to 1.4mmol/L in cats. Serum iCa concentrations in younger dogs and cats are, on average, 0.025mmol/L to 0.1mmol/L higher than adults.
Mild iHCa (0.9mmol/L to 1.1mmol/L) – as seen in critically ill dogs and cats with diabetic ketoacidosis, acute pancreatitis, protein-losing enteropathies, sepsis, trauma, tumour lysis syndrome or urethral obstructions – often has no observable clinical signs.
Moderately (0.8mmol/L to 0.9mmol/L) to severely (lower than 0.8mmol/L) affected animals – in the case of eclampsia and those with parathyroid disease – often display severe signs.
Early signs of iHCa are often non-specific, and include:
anorexia
rubbing of the face
agitation
restlessness
hypersensitivity
stiff and stilted gait
As the serum iCa concentration further decreases, patients often progress to:
paresthesia
tachypnoea
generalised muscle fasciculations
cramping
tetany
seizures
In cats, the gastrointestinal system can also be affected, presenting as anorexia and vomiting.
Treatment
The need for treatment of hypocalcaemia is dependent on the presence of clinical signs, rather than a specific cut-off of serum concentration of iCa itself.
Moderate to severe iHCa should always be treated. Mild hypocalcaemia, on the other hand, may not be necessary, especially if it is well tolerated. It should be remembered the threshold for development of clinical signs is variable, and treatment may benefit critical cases with an iCa concentration of less than 1.0mmol/L.
Treatment is divided into the acute treatment phase and chronic management.
In the tetanic phase, IV calcium is required – 10% calcium gluconate (equivalent to 9.3mg/ml) administered at 0.5ml/kg to 1.5ml/kg dosing to effect. This should be administered slowly with concurrent ECG monitoring. Infusion of calcium needs to be stopped if bradycardia develops or if shortening of the QT interval occurs.
Some suggest calcium gluconate (diluted 1:1 with 0.9% sodium chloride) of half or the full IV dose can be given SC and repeated every six to eight hours until the patient is stable enough to receive oral supplementation. However, be aware calcium salts SC can cause severe necrosis or skin mineralisation.
Calcium chloride should never be given SC, as it is a severe perivascular irritant.
Correcting iCa
Irrespective of the chronicity of the treatment, the rule of thumb is correction of calcium should not exceed 1.1mmol/L.
Correction of iCa to normal or hypercalcaemic concentration should always be avoided, as this will result in the desensitisation of the parathyroid response, predisposing renal mineralisation and formation of urinary calculi.
Some of the more common calcium supplementation medications – both parenteral and oral formulas – are detailed in Table 1. Supplementation of magnesium may also benefit some patients, as it is a common concurrent finding in critically ill patients with iHCa.
Table 1. Common calcium supplementation medications
Drug
Calcium Content
Dose
Comment
Parenteral calcium
Calcium gluconate
(10% solution)
9.3mg/ml
i) slow IV dosing to effect (0.5ml/kg to 1.5ml/kg); acute crisis, 50mg/kg to 150mg/kg over 20 to 30 minutes
ii) 5mg/kg/hr to 15mg/kg/hr IV or 1,000mg/kg/day to 1,500mg/kg/day (or 42mg/kg/hr to 63mg/kg/hr)
Stop if bradycardia or shortened QT interval occurs.
Infusion to maintain normal Ca level
SC calcium salts can cause severe skin necrosis/mineralisation.
Calcium chloride
(10% solution)
27.2mg/ml
5mg/kg/hr to 15mg/kg/hr IV
Do not give SC as severe perivascular irritant
Oral calcium
Calcium carbonate
(many sizes)
40% tablet
5mg/kg/day to 15mg/kg/day
Calcium lactate
(325mg, 650mg)
13% tablet
25mg/kg/day to 50mg/kg/day
Calcium chloride
(powder)
27.2%
25mg/kg/day to 50mg/kg/day
May cause gastric irritation
Calcium gluconate (many sizes)
10%
25mg/kg/day to 50mg/kg/day
Next time…
The next blog will look at the pathophysiology behind iHCa among critically ill animals. It will also look at the controversy regarding treatment of non-clinical iHCa cases and the prognostic indications of iCa concentrations.
Postoperatively, gastric dilatation-volvulus (GDV) patients remain in our intensive care unit for at least two to three days.
Monitoring includes standard general physical examination parameters, invasive arterial blood pressures, ECG, urine output via urinary catheter and pain scoring.
I repeat PCV/total protein, lactate, blood gas and activated clotting times (ACT) immediately postoperatively and then every 8-12 hours, depending on abnormalities and patient progress.
Patient recovering in the pet intensive care unit. As well as standard monitoring parameters, GDV patients have constant ECG, arterial blood pressure and urine output monitoring to enable the early detection and correction of abnormalities.
I always repeat these blood tests postoperatively, as IV fluids given during the resuscitation and intraoperative period often cause derangements. I use the results to guide my fluid therapy, but also take it with a grain of salt.
IV fluids
I generally continue a balanced and buffered crystalloid. The rate depends on blood pressures, urine output and assessment of general physical examination parameters for perfusion and hydration, but I try to avoid fluid overload and reduce the IV fluids postoperatively as soon as possible.
Coagulopathy
Prolonged clotting times are frequently seen as a result of consumption in a dog with GDV. However, one should note it can also occur as the result of haemodilution.
As the underlying disease process has been corrected, and haemostasis achieved during surgery, I usually monitor ACTs, but may not necessarily treat with blood products as prolonged ACTs do not always translate to clinical bleeding. Unless clinical evidence of bleeding exists, I generally hold off treatment and monitor.
Hypoproteinaemia
Low total protein is also common. This is generally due to haemodilution from fluid resuscitation. However, a low total protein does not mean oedema will develop, or that it requires management. I generally track the protein levels, use conservative fluid therapy and try to correct it by instituting enteral nutrition as soon as possible.
Electrolyte imbalances
Hypokalaemia is a common complication of fluid therapy. This can be rectified with potassium supplementation in the IV fluids.
Hyperlactataemia
If present post-surgery, this is usually corrected with a fluid bolus. However, I always assess for other things that may affect oxygen delivery to the tissues, such as poor cardiac output (arrthymias), hypoxaemia (respiratory disease) and anaemia (from surgical blood loss).
Arrhythmias
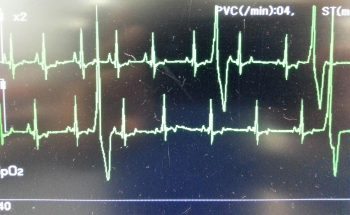
Ventricular arrhythmias are common post-surgery. Accelerated idioventricular rhythms are the most common cause, especially if a splenectomy was performed.
Ventricular premature contractions are common postoperative arrhythmia.
Before reaching for anti-arrythmia medications, first check and correct:
electrolyte abnormalities
hypoxaemia
pain control
hypovolaemia or hypotension
If they are still present, despite correction of the above, consider treating the rhythm if:
multifocal beats (ventricular premature contractions of various sizes)
overall rate greater than 190 beats per minute
R-on-T phenomenon
low blood pressure during a run of ventricular premature contractions
I start with a bolus 2mg/kg lidocaine IV and start a constant-rate infusion of 50ug/kg/min to 75ug/kg/min.
Anaemia
It is common to have a mild anaemia post-surgery, due to a combination of blood loss and haemodilution. In the absence of transfusion triggers – such as increased heart rate, increased respiratory rate or hyperlactataemia – it does not require treatment.
Vomiting
Anti-emetics are the first line of medication. Non-prokinetic anti-emetics, such as maropitant and ondansetron, can be used immediately; otherwise, after 12 hours, metoclopramide can also be used postoperatively. If the patient remains nauseous despite these medications, the placement of a nasogastric tube can ease nausea by removing static gastric fluid.
Excessive pain relief may also contribute to the nauseous state.
Pain relief
I mostly rely on potent-pure opioid agonists, such as fentanyl constant-rate infusions and patches. This is generally sufficient for most patients. Ketamine is occasionally used.
Some drugs listed in this article are used under the cascade.
Christmas can be a busy time for vet clinics, so here is a list of common intoxications and conditions to keep an eye out on during the festive period.
Chocolate
Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.
I always perform emesis in patients that have ingested chocolate, even hours after ingestion as often large amounts can reside in the stomach.
Remember that cardiac arrhythmias can also occur in clinically normal looking patients, so perform an ECG.
The toxic components can be reabsorbed through the bladder wall; therefore, urinary catheterisation is a part of management of this intoxication.
Onions
Onions used in roasts and on BBQ’s can cause Heinz body formation, haemolytic anaemias and pigmenturia.
This is not a common intoxication, but should be considered in anaemia patients and those with discoloured urine.
Raisins
Commonly used in Christmas cakes and puddings. They can cause acute kidney failure, the exact mechanism of action is unknown, and there does not appear to be a dose-dependent relationship.
It should always be a differential for azotemic patients this time of year.
IV fluid induced diuresis for 48 hours is the safest way to manage raisin exposure.
Mistletoe
The berries can be fatal, even if only a couple are ingested.
Ethylene glycol
In colder climates, ethylene glycol can be a very common toxicity.
This sweet liquid is very attractive to pets and can cause acute renal failure, with the first signs being acute onset ataxia.
Macadamia nuts
Macadamia nuts are common in some parts of the world. They result in joint pain in the hocks and carpus leading to weakness and ataxia.
Often confused with trauma and soft tissue injuries. Hyperextension of the hocks and sometimes flexion of the carpus are the clinical features.
Xylitol
Xylitol is a sugar-free product used in lollies and baking.
In dogs, it triggers endogenous insulin to be released and a subsequent hypoglycemia develops. It can also cause hepatic failure.
As a general rule, I approach all intoxications as if they could be fatal as it is rare to know exactly how much of the toxic agent they have been exposed to. I consider if a patient I am treating for intoxication never develops clinical signs and wonder whether it was going to or not is the best outcome.
Strings
Look under the tongue.
Linear foreign bodies can be difficult to diagnose. Some features on abdominal radiographs to look out for include abnormal bunching of the small intestines, and “c” and “comma” shaped gas patterns.
Christmas meals
Gastroenteritis is the most common presenting condition over the Christmas period, with dietary change and indiscretion often being the culprit.
Bones can lead to obstructions from oral cavity to the intestines and can also cause constipation.
Leftover meat trimmings, often fat laden, are a common cause of pancreatitis.
BBQ skewers
In some parts of the world (Australia especially) BBQs are common around Christmas time.
BBQ skewers can cause gastrointestinal tract perforation and septic peritonitis.
Because they are not radiopaque they are often difficult to diagnose.
Gastric dilatation-volvulus (GDV) is a true veterinary emergency and while it can be daunting to be presented with a sick dog with suspected GDV, the most important thing to remember is this patient will likely succumb to this condition without your intervention.
First, a little pathophysiology: GDV is a broad term that can refer to gastric dilation on its own, gastric dilation with volvulus, and even chronic gastric volvulus. These conditions usually present in large or giant breeds and we still know little about the underlying causes.
Gastric dilatation-volvulus (click to zoom).
Once dilation and volvulus occurs, perfusion to the stomach and other abdominal organs is compromised. Along with general shock – which can be fatal in its own right – decreased stomach wall perfusion can result in stomach wall necrosis, rupture and peritonitis.
Clinical signs
Quite often, a GDV case starts with a telephone call from a panicking owner. He or she usually reports an acute onset of retching, regurgitation or vomiting in their large or giant breed dog after feeding.
Other common signs include:
hypersalivation
agitation
palpable abdominal distension
When presented, many of these cases will be obvious and the animal already in some degree of shock. You need to institute fluid resuscitation and gastric decompression immediately to restore perfusion as soon as possible.
Confirmation
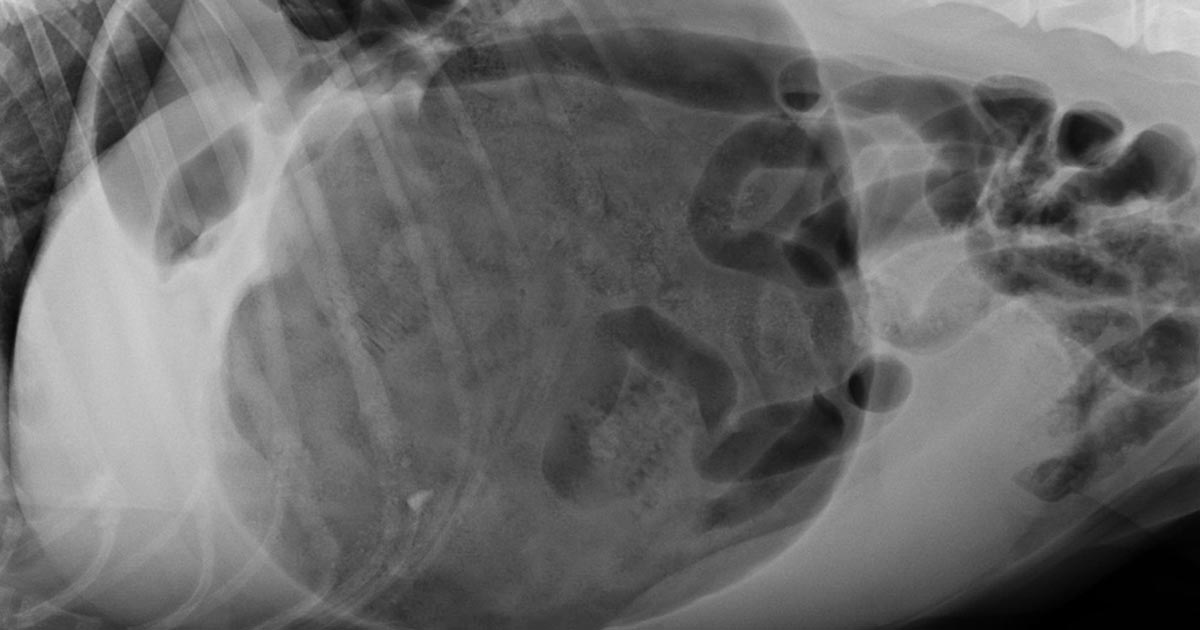
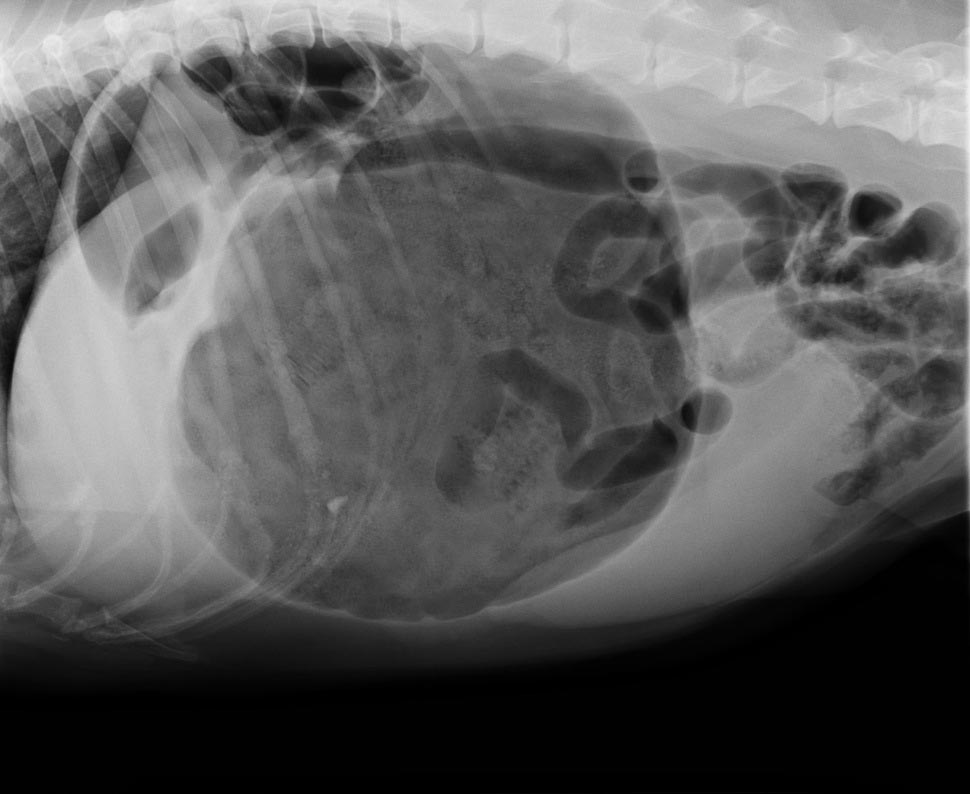
To confirm the patient truly has GDV, as some patients may present with simple gastric dilation from over-engorgement, you need to perform an abdominal radiograph.
Always keep an eye out for the large, deep-chested dog that presents with vomiting or retching, but doesn’t appear bloated. Don’t be fooled into ruling out GDV in these patients based on physical examination alone – often, no visible or palpable gastric distension exists as the ribs cover the stomach. That is where the abdominal radiographs play an especially important role.
It is common practice at our hospital to perform abdominal radiographs as soon as possible, so as to not miss a hidden or subtle GDV in these large breed dogs.
Which view is best?
The classic approach is to lie the patient in right-lateral recumbency, in this view, you would see the classic “Smurf’s hat”, “boxing glove”, “Popeye’s arm”, “double bubble”, etc. This is compartmentalisation of the stomach, indicating not only gastric dilatation, but volvulus as well.
You should also look for evidence of pneumoperitoneum, as it may suggest gastric wall rupture.
At this stage, it is also important to collect blood for biochemistry, haematology, electrolytes and, if available to you, blood gas analysis. ECG readings should also be taken to determine if the patient has any life-threatening arrhythmias, such as ventricular tachycardia.
Next month, we will talk about stabilising and treating these patients.



 Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.
Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.