Great news for those who hate enemas: you may not have to do any of these ever again. This is the consensus by both the American Academy of Clinical Toxicology, and the European Association of Poisons Centres and Clinical Toxicologists.
The theory behind these procedures is legitimate – reducing systemic exposure of a toxicant by accelerating gastrointestinal tract (GIT) expulsion. But this is assuming the toxicant is absorbed very slowly, undergoes substantial enterohepatic cycling, or undergoes slow reabsorption in the lower GIT – all of which are uncommon characteristics of the types of toxicants veterinary patients are exposed to.
In fact, most toxicants of veterinary interests are generally rapidly absorbed in the upper GIT and absorption are not affected by catharsis.
Lack of evidence
No clinical evidence exists to support the use of a cathartic alone, or in combination with activated charcoal, to reduce the bioavailability of drugs or to improve the clinical outcome of poisoned patients. In fact, some evidence shows systemic exposure is increased following oral dosing of sorbitol, with activated charcoal, in canine paracetamol poisoning cases.
Similarly, no evidence exists that enemas and/or colonic irrigation improve clinical outcome in the treatment of oral poisoning.
The risks can be quite high with these procedures, with patients at risk of:
haemorrhage (in the case of anticoagulant vitamin K antagonist rodenticides, for example)
electrolyte destabilisation
bowel perforation
rectal prolapse
phosphate toxicities (cats)
The risks simply do not outweigh the benefit (or lack thereof). In fact, repeated dosing with combination preparations containing sorbitol and activated charcoal is not recommended.
This may be the most exciting news in veterinary medicine!
When interpreting the often misinterpreted and underused PCV and total solids test, it is important to take note of the serum colour as this may give clues into the diagnosis.
Normal serum colour (left) compared to a patient with immune-mediated haemolytic anaemia. The serum is haemolysed and anaemia is present.
The most common abnormalities seen in clinic are icteric, haemolysed and lipaemic serum.
Clear serum can also be of importance – especially when you interpret it with blood counts and urine colour.
Haemolysis
The most common abnormality of serum colour changes is haemolysis. In my experience, the most common cause is suboptimal collection technique. To confirm this, simply collect another sample and repeat.
If it is repeatable, and concurrent anaemia or pigmenturia is present, it warrants further investigation.
Intravascular haemolysis can be caused by:
immune-mediated haemolytic anaemia
blood transfusion reactions
infectious diseases such as Mycoplasma haemofelis, Babesia canis, Ehrlichia canis, FeLV and others
Heinz bodies from the ingestion of heavy metal, onions or paracetamol
hypophosphataemia
macroangiopathic disease (neoplasia, for example)
envenomation – typically, snake bites
Testing issues
Haemolysis can also affect other laboratory testing. It can lead to an artefactual increase in glucose, phosphorus, bilirubin, total protein, fructosamine and triglycerides, and a decrease in sodium (pseudohyponatraemia), cholesterol, calcium, potassium and albumin.
Extravascular haemolysis often does not cause haemolysed serum as it is generally slower and the body is able to clear the haemoglobin before it can lead to discolouration of the serum.
Euthanasia is a big part of our work as veterinarians. Working in an emergency setting, it is something I have to face on every shift.
It doesn’t get any easier no matter how many times I have to do it, but I have fine-tuned my approach over the years so each euthanasia process runs as smoothly as possible, with minimal additional stress to both patient and client.
This month, I will talk about taking care of your client.
Communication is key
Euthanasia is a big part of our work as veterinarians.
The most important aspect of taking care of your client in this difficult time is to make sure you really focus on communicating clearly, effectively and, most importantly, with sincere empathy.
First, I listen to their concerns, and why they have made the difficult decision to euthanise their pet.
Quality of life decisions can be a very grey area, and sometimes what you think may be manageable as a veterinarian can be a huge quality of life concern for a pet owner.
A prime example is osteoarthritis in older dogs. You may assess them as being clinically well except for some difficulty walking, but the client sees their pet every day and notices the struggles they go through.
Euthanasia is a difficult conclusion for them to come to and, in most instances, I will defer to the client when it comes to assessing the quality of life of their pet.
Quality assessment
One way I help clients assess their pet’s quality of life is by asking them about a few aspects of it, including:
Can your pet do the things that make them happy?
Do they spend more days sad, depressed and ill compared to the number of days they are bright, happy and eating?
Is your pet in pain? Is this pain manageable?
Confirmation
Once a client has expressed they want to euthanise their pet, I always try to confirm three things:
That they have actually decided to euthanise their pet. I frame the question like: “So, my understanding from our conversation is that you have made the decision to euthanise Fluffy today?” Sometimes, when you ask this question, the client reveals they have not actually come to that decision yet, which means you will need to backtrack a little and guide them through the decision process again.
Whether they would like to be present for the euthanasia.
How they would like us to handle the after care.
I also always try to manage all documentation and finances before the euthanasia so the clients will be in a position to leave immediately after the procedure, meaning they can begin to grieve rather than have to do paperwork. The only exception to this is when the patient is in a critical condition, meaning euthanasia cannot wait.
Explaining the process
Try not to perform the euthanasia in your consult room or in the main treatment areas – if you have a private room for euthanasias, that is the most ideal. This is important especially if the client comes back in the future with another pet or a new pet. They often find it difficult to walk into your consult room and be reminded of the euthanasia of their beloved pet.
I like to give clients some time to spend alone with their pet to say their goodbyes in private. When I come back into the room, I start by explaining the process of the euthanasia, covering the following things every single time:
Euthanasia is an overdose of an anaesthetic agent
The process is quick – 10 to 20 seconds
It is completely painless
The pet doesn’t close their eyes afterwards
The pet can have a couple deep breaths and muscle tremors
The pet can release their bowels and bladder (especially important to warn of this if the clients want to hold their pet)
Lastly, if their pet came into the hospital in shock and obtunded, where I have fluid resuscitated them, meaning they are now more bright and alert, I warn the clients that despite their pet looking better, the underlying disease remains the same.
Once the euthanasia is performed, I again ask if the client wants to spend a little more time in private with their pet. Finally, when the client leaves, they typically will say “thank you”.
Whatever you do, do not say something like “my pleasure” or “you’re welcome” like you would for a vaccination consult – this is a natural response, but would be a terrible faux pas. I simply say “I’m very sorry for your loss. Take care for now and let us know if we can help in any way”.
Next month, I will talk about taking care of your patient throughout the euthanasia process.
Now we cover the three things you need to do as soon as a suspected case is presented:
IV fluid resuscitation
decompression of the stomach
pain relief
Depending on the number of staff you have, all of these can be performed simultaneously. If not, follow the above order as shock is the most imminent problem.
Catheter placement
Fluid resuscitation is relatively straightforward. Most GDV patients will be in some degree of shock, varying from mild to severe. Regardless of the actual degree, all patients will require IV fluids.
The placement of IV catheters is particularly important; their numbers and diameter will influence the rate of response to treatment. Large-bore catheters allow faster flow of fluids compared to smaller ones, while multiple catheters allow concurrent delivery of two bags of fluids as opposed to one – particularly important in large dogs. Therefore, always try to place the largest catheter possible (for example, 18G or larger for large-breed dogs) into the cephalic veins.
Once the catheters have been placed, collect 2ml to 3ml of blood for baseline measurements. These can be collected directly from the catheters and should include:
PCV/total protein
blood gas analysis
lactate
activated clotting time
electrolytes
later, full haematological and biochemical analysis
Once the baseline bloods have been collected, fluid resuscitation should start immediately.
How much, how fast?
Fluid resuscitation is relatively straightforward, says vet Gerardo Poli.
How much fluid should you deliver, and how fast? My “go to” fluid is crystalloids and I generally start with a 20ml/kg bolus of an alkalinising crystalloid.
I perform bolus therapy, so 10ml/kg to 20ml/kg fluid doses rather than shock rates 90ml/kg/hr, as I feel it allows me to better titrate my fluid therapy to effect. It also helps minimise excessive fluid administration and the problems with haemodilution – such as anaemia, hypoproteinaemia and prolonged coagulation times.
As fluids are being delivered, I administer pain relief and start gastric decompression (covered next week).
The decision to administer more fluids depends on whether I have achieved some end point resuscitation variables, such as:
a reduction in heart rate
a reduction in capillary refill time
an improvement of mucus membrane colour
improvement in pulse pressures
Improvement in mentation is not often reliable as the sedative effect of analgesia, which I generally give during fluid resuscitation, often confounds this effect.
Shock therapy
If evidence of shock still exists, despite the initial fluid boluses and gastric decompression, I will consider more fluids. This can include hypertonic saline or colloids.
In my experience, a repeat of a smaller dose of crystalloid fluid bolus is often adequate (10ml/kg). The transition on to hypertonic saline (7% solution) or colloids is influenced by the results of the aforementioned baseline diagnostics.
A reduction in PCV/total protein suggests blood loss. In this case, I will consider either hypertonic saline (3ml/kg to 5ml/kg of 7% solution), a dose of colloids or even blood products, such as whole blood or packed red blood cells.
If significant prolongation in activated clotting time occurs, likely from consumption, then I may incorporate fresh frozen plasma into my fluid therapy. This is in anticipation of possible surgery, where prolonged coagulation times can not only be troublesome, but life-threatening.
Lactate
A quick note on lactate – I don’t use the baseline reading as a prognostic indicator or an indicator of gastric necrosis. This is supported by recent findings claiming it is not the level of lactate that is predictive, but the degree of improvement in response to fluid resuscitation and gastric decompression.
I have seen unreadable lactate levels – greater than 15mmol/L – in patients who returned to reasonably normal levels within an hour of stabilising. These patients also went on to survive surgery.
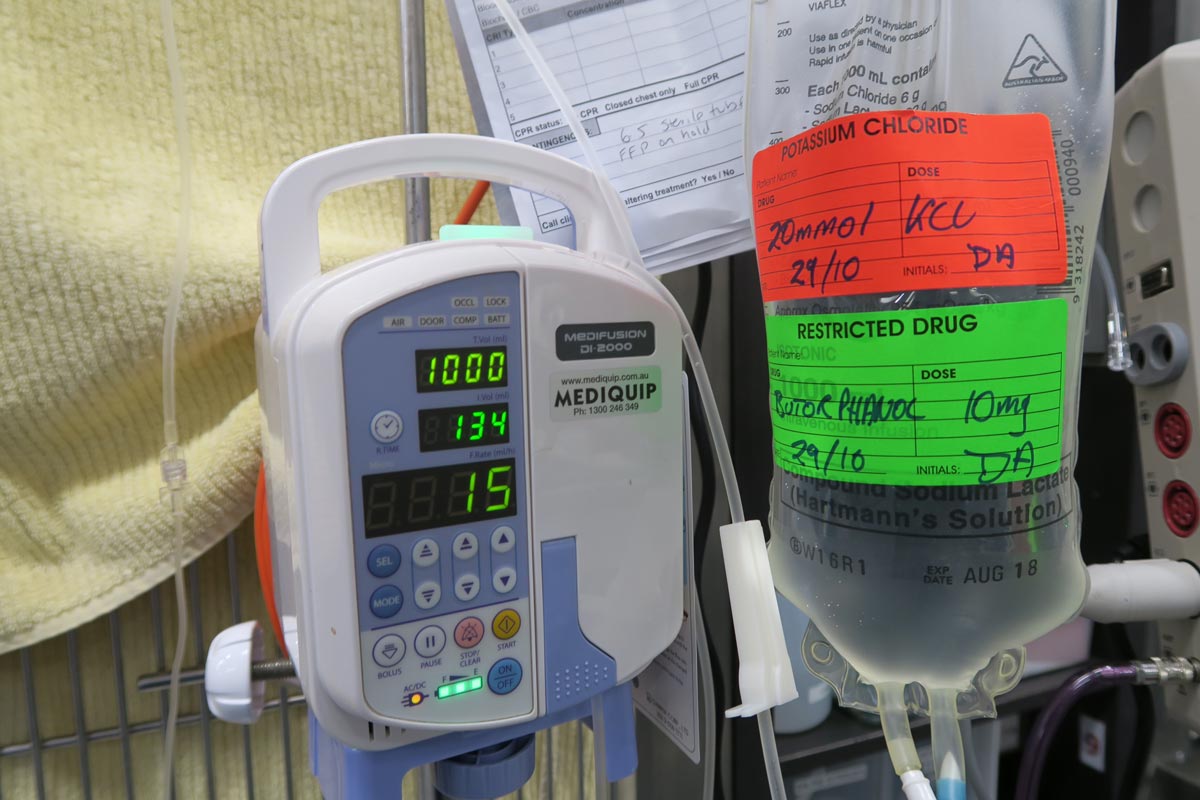
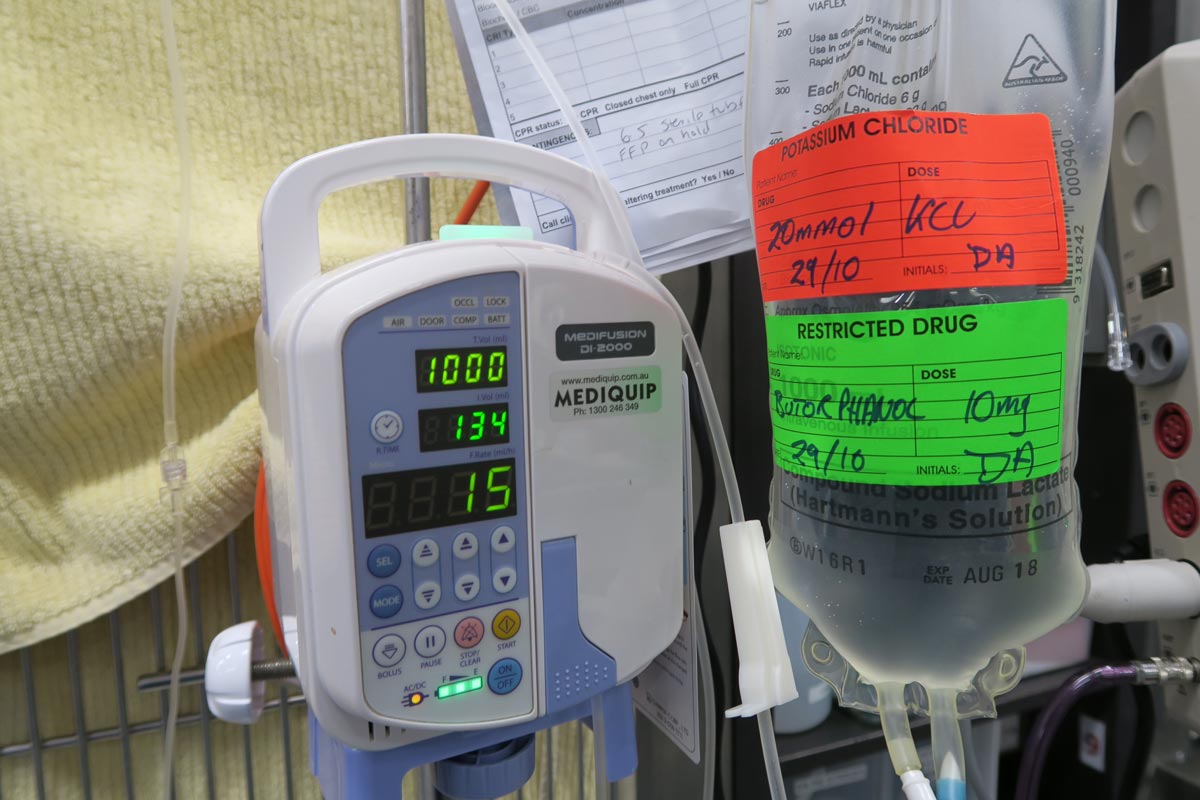
Pain relief
After starting IV fluid resuscitation, I generally administer pain relief while the team is preparing for gastric decompression. To keep things simple, I stick to an easily accessible pure opioid agonist at 0.2mg/kg IV. I avoid subcutaneous or even intramuscular administration as the patient is often in shock; the peripheral blood is shunted centrally to the heart and the brain and absorption can be variable.
I find this offers a reliable and great degree of pain relief that helps reduce anxiety levels and, consequently, reduces oxygen demand. It has minimal cardiovascular effects and the mild sedative effect also helps with the process of decompression.
Christmas can be a busy time for vet clinics, so here is a list of common intoxications and conditions to keep an eye out on during the festive period.
Chocolate
Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.
I always perform emesis in patients that have ingested chocolate, even hours after ingestion as often large amounts can reside in the stomach.
Remember that cardiac arrhythmias can also occur in clinically normal looking patients, so perform an ECG.
The toxic components can be reabsorbed through the bladder wall; therefore, urinary catheterisation is a part of management of this intoxication.
Onions
Onions used in roasts and on BBQ’s can cause Heinz body formation, haemolytic anaemias and pigmenturia.
This is not a common intoxication, but should be considered in anaemia patients and those with discoloured urine.
Raisins
Commonly used in Christmas cakes and puddings. They can cause acute kidney failure, the exact mechanism of action is unknown, and there does not appear to be a dose-dependent relationship.
It should always be a differential for azotemic patients this time of year.
IV fluid induced diuresis for 48 hours is the safest way to manage raisin exposure.
Mistletoe
The berries can be fatal, even if only a couple are ingested.
Ethylene glycol
In colder climates, ethylene glycol can be a very common toxicity.
This sweet liquid is very attractive to pets and can cause acute renal failure, with the first signs being acute onset ataxia.
Macadamia nuts
Macadamia nuts are common in some parts of the world. They result in joint pain in the hocks and carpus leading to weakness and ataxia.
Often confused with trauma and soft tissue injuries. Hyperextension of the hocks and sometimes flexion of the carpus are the clinical features.
Xylitol
Xylitol is a sugar-free product used in lollies and baking.
In dogs, it triggers endogenous insulin to be released and a subsequent hypoglycemia develops. It can also cause hepatic failure.
As a general rule, I approach all intoxications as if they could be fatal as it is rare to know exactly how much of the toxic agent they have been exposed to. I consider if a patient I am treating for intoxication never develops clinical signs and wonder whether it was going to or not is the best outcome.
Strings
Look under the tongue.
Linear foreign bodies can be difficult to diagnose. Some features on abdominal radiographs to look out for include abnormal bunching of the small intestines, and “c” and “comma” shaped gas patterns.
Christmas meals
Gastroenteritis is the most common presenting condition over the Christmas period, with dietary change and indiscretion often being the culprit.
Bones can lead to obstructions from oral cavity to the intestines and can also cause constipation.
Leftover meat trimmings, often fat laden, are a common cause of pancreatitis.
BBQ skewers
In some parts of the world (Australia especially) BBQs are common around Christmas time.
BBQ skewers can cause gastrointestinal tract perforation and septic peritonitis.
Because they are not radiopaque they are often difficult to diagnose.
Until I started researching this Tip of The Week, I did not know the medical profession has abandoned the routine use of emesis in oral poisoning.
This is based on multiple medical literatures that have proven emesis induction does not influence the clinical severity of poisoning, the length of hospitalisation and the clinical outcome or mortality.
Although the rationale for inducing emesis is obvious, it is not necessarily evidence based. It is also dependent on satisfying a few large assumptions, all of which are untrue:
Emesis is a very effective way of removing gastric contents.
No separation exists of poison from its vehicle while inside the acidic environment of the stomach.
Poison is not absorbed through the stomach wall.
Ineffective method
Snail bait ingestions: this patient ate 500g of snail bait containing metaldehyde.
Emesis induction is an ineffective way of clearing stomach contents. A review of the effectiveness of induced emesis, with both human and canine participants, showed at 30 minutes post-ingestion of non-absorbable markers, the recovery rate averaged between 17.5% and 52.1%, but never exceeded 62%.
In fasted puppies, this was even lower at 2% to 31%, despite inducing emesis immediately after marker administration. These have been confirmed by the presence of poisonous materials in the stomach of dead patients, despite effective emesis induction until clear fluid was brought up.
The clinical outcome only improves if the systemic exposure of a toxicant is reduced by more than half. However, considering animals rarely practice restraint, the ingested amount is unlikely to be exactly the lethal dose and no more. Therefore, even reducing the ingested toxic dose by 62% is unlikely to make a clinical difference.
Furthermore, most patients rarely present within 30 minutes of ingesting a toxicant, thus further reducing its efficiency.
The absorption conundrum
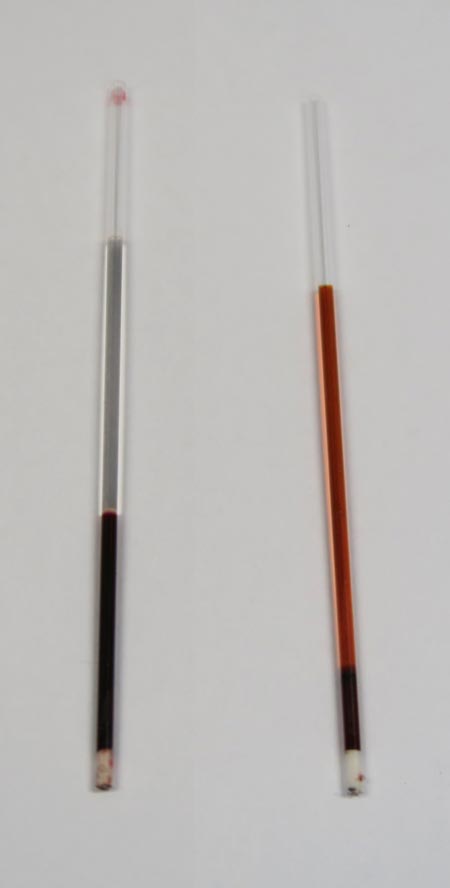
Some may argue the retrieval of metaldehyde or anticoagulant rodenticide granules from vomitus is indicative of reducing the toxicant dose. This could be true, but only if emesis was induced immediately after ingesting the poison.
The poison itself is colourless and has a different absorption characteristic to the coloured vehicle (granule); therefore, the presence of granule only serves to confirm ingestion, but is of no indication whether the poison has already been absorbed.
Contraindications
Many well-recognised absolute contraindications also exist to inducing vomiting:
Ingestion of oils, which includes waxes that melt to oil in the internal body environment, as this poses a high risk of lipoid and bacterial pneumonia. This is of significant veterinary significance, as wax is routinely used in rodenticide baits.
Ingestion of hydrocarbons and other volatile substances, or caustic or corrosive substances.
When the mental status is altered – for example, hyperexcitable or depressed mental state.
Where the patient is at risk of seizures (seizures can be induced by emesis).
Increased intracranial pressure.
Risk of intracranial or cerebral haemorrhage – for example, thrombocytopenia or abnormal clotting parameters.
Other less severe, yet important, reasons include:
delays administration of more effective treatment, such as activated charcoal, antidote or other treatments
risk of aspiration pneumonia
hypochloraemia in recurrent emetic patients
significant CNS and respiratory depression from apomorphine
rare, but reported, complications such as cerebral haemorrhage, oesophageal tear/ rupture, hiatal hernia, gastric rupture, pneumothorax and pneumomediastinum
legal implications – for example, if the product information clearly states emesis should not be induced
A place for everything
Emesis induction is not a benign procedure. It still has its place in certain circumstances, but its use in the routine management of oral poisonings may need to be reconsidered – especially if it means delaying administration of a more effective treatment, such as activated charcoal.
So, after all this, how do I tackle this information? It is a bit hard to swallow. My clinical experience is emesis is generally safe, especially in canine patients using apomorphine. So, I still feel some merit exists in reducing the amount of toxicant in the stomach if you have a chance – and in some situations, you don’t know until you try.
Emesis after ingestion of a toxic dose of chocolate can be incredibly rewarding, even six hours after ingestion, leading to patients not developing clinical signs at all.
Overall, I am biased by my personal successes with emesis, so still feel a time and place exist for emesis induction. But I now stop and question my decision to induce emesis, whereas I did not hesitate before.
Gastric dilatation-volvulus (GDV) is a true veterinary emergency and while it can be daunting to be presented with a sick dog with suspected GDV, the most important thing to remember is this patient will likely succumb to this condition without your intervention.
First, a little pathophysiology: GDV is a broad term that can refer to gastric dilation on its own, gastric dilation with volvulus, and even chronic gastric volvulus. These conditions usually present in large or giant breeds and we still know little about the underlying causes.
Gastric dilatation-volvulus (click to zoom).
Once dilation and volvulus occurs, perfusion to the stomach and other abdominal organs is compromised. Along with general shock – which can be fatal in its own right – decreased stomach wall perfusion can result in stomach wall necrosis, rupture and peritonitis.
Clinical signs
Quite often, a GDV case starts with a telephone call from a panicking owner. He or she usually reports an acute onset of retching, regurgitation or vomiting in their large or giant breed dog after feeding.
Other common signs include:
hypersalivation
agitation
palpable abdominal distension
When presented, many of these cases will be obvious and the animal already in some degree of shock. You need to institute fluid resuscitation and gastric decompression immediately to restore perfusion as soon as possible.
Confirmation
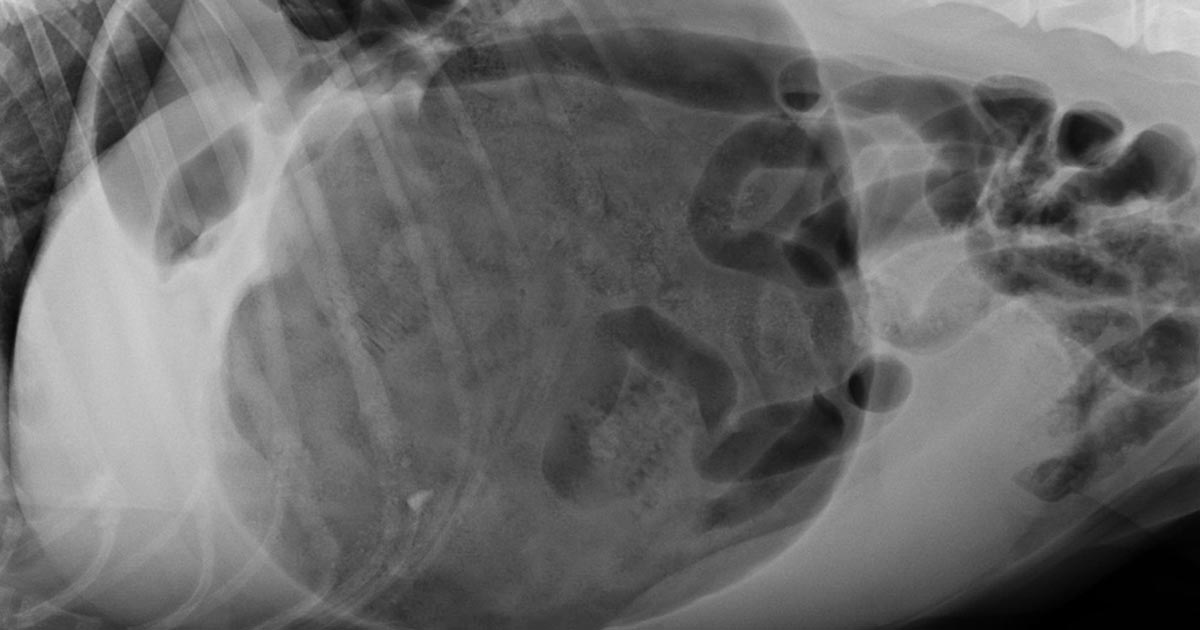
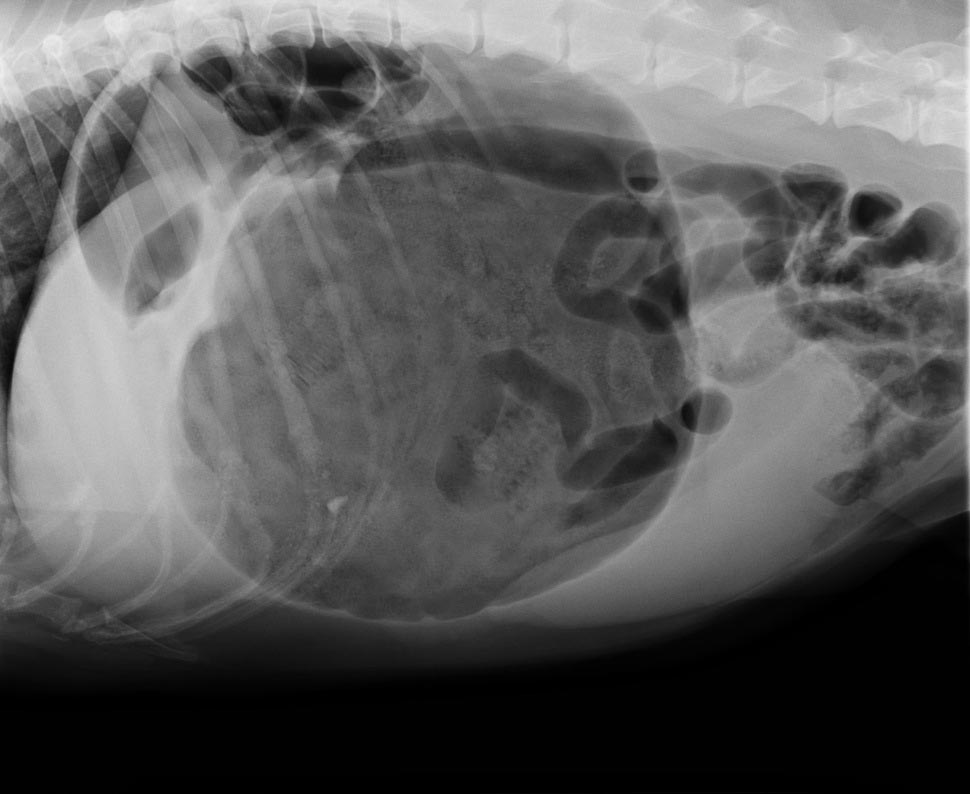
To confirm the patient truly has GDV, as some patients may present with simple gastric dilation from over-engorgement, you need to perform an abdominal radiograph.
Always keep an eye out for the large, deep-chested dog that presents with vomiting or retching, but doesn’t appear bloated. Don’t be fooled into ruling out GDV in these patients based on physical examination alone – often, no visible or palpable gastric distension exists as the ribs cover the stomach. That is where the abdominal radiographs play an especially important role.
It is common practice at our hospital to perform abdominal radiographs as soon as possible, so as to not miss a hidden or subtle GDV in these large breed dogs.
Which view is best?
The classic approach is to lie the patient in right-lateral recumbency, in this view, you would see the classic “Smurf’s hat”, “boxing glove”, “Popeye’s arm”, “double bubble”, etc. This is compartmentalisation of the stomach, indicating not only gastric dilatation, but volvulus as well.
You should also look for evidence of pneumoperitoneum, as it may suggest gastric wall rupture.
At this stage, it is also important to collect blood for biochemistry, haematology, electrolytes and, if available to you, blood gas analysis. ECG readings should also be taken to determine if the patient has any life-threatening arrhythmias, such as ventricular tachycardia.
Next month, we will talk about stabilising and treating these patients.
Every vet has their niche, speciality or personal interest. I think I’m slowly finding that mine may be located somewhere in the gastrointestinal (GI) system; as the daughter of an endoscopy nurse I like to think I’m following in the family footsteps.
I was really enjoying my lectures on the topic until we reached the point of hiatal hernias.
The unfortunate cognitive dissonance of veterinary medicine is that the more interesting or objectively “cooler” the case, the more likely it is often incredibly sad from the perspective of the patient.
Vet geek
In this case, I personally was finding the concept of a sliding hernia pretty “cool” (don’t judge, I’ve been out of the game for a year and I’ve missed nerding out over-vetty stuff), until I learned that the majority of brachycephalic dogs suffer from the condition.
The mechanism behind this being that, in an effort to breathe through an actively collapsing airway, a brachycephalic dog can effectively create such a negative pressure that it sucks its stomach through its diaphragm and into its thorax.
The worst part of this is that it’s suspected the majority of cases are subclinical (or, at least, subclinical to the owner), as the main clinical signs associated with nausea, such as drooling and lip smacking, are characteristic of short-nosed breeds anyway.
Less love?
I wonder if a pilot finds it impossible to enjoy a flight? Even if you stuck him in first class with a martini, the Friends box set, comfy slippers and a sirloin steak on the menu, would he be able to switch off, or would he find his mind focusing on minute turbulence? Would he keep checking the altitude, or picturing the cockpit, wondering: “What on Earth is going on up there?”
Along a similar vein, by the time I finish vet school I wonder if I will ever be able to truly enjoy a dog in the way I used to? If somebody had presented me with the fluffiest, most adorably friendly puppy in the world the day before I’d started first year, I’d have been ecstatic – I may even have passed out from happiness.
Not just a puppy
Now, don’t get me wrong, I’m never NOT going to love being handed a puppy, but it’s not just a puppy anymore.
Has it been vaccinated?
Was its mother healthy?
Did the breeder socialise it effectively, or will it forever have a fear of bearded men in funny hats?
Is there a cleft palate behind those tiny teeth?
Are there worms lurking in that adorable pot belly?
It’s like my subconscious races to take a history in every animal – even if they’re not a patient!
Natural versus artificial selection
As a constant reminder of my disturbing lecture notes, while tutoring GCSE biology I regularly cover the topic of “natural versus artificial selection” with my students. This includes covering the staggering feet of man’s journey over the past 1,000 years to convert the wolf into anything from a small bear to something that fits in a handbag.
Each time I teach this topic I find myself fighting the urge to be overly pious, knowing no exam will ever ask them to list the ways the pug is destined to a snorting existence or why the dachshund can’t jump onto his owner’s lap for fear of shattering his spine.
I feel including that sort of thing in the syllabus could certainly go a long way – and perhaps the best way to promote healthy dogs is with re-education from the ground up. But is that my responsibility? More importantly, is it the responsibility of vets in general?
Flawed from birth
With some owners (especially breeders), mentioning any predispositions or hereditary conditions of their dog is akin to attacking their personal brand.
Some people are “dog people”, while some are very passionately and unequivocally only “pug people” or “sausage dog people” or “golden people” – and it’s generally a struggle not to cause offense when telling an owner their animal is slightly overweight, let alone that their pride and joy is genetically predisposed to be flawed from birth.
The frustrating thing is that if owners knew the risks to their particular pup then prophylactic management could really make a difference to these animals’ lives.
Not walking brachycephalic breeds on hot days, keeping the weight off of larger dogs to take the stress off of their joints – prevention is always better than cure, and if we can’t prevent the breeding and purchasing of puppies with a gene pool so shallow only a gnat could drown in it then at the very least we should be aiming to prevent suffering and promoting comfort.
Balancing act
The danger, as always, is that if you tell an owner what they don’t want to hear too many times, they won’t come back. So, the balancing act lies in maintaining the client-vet relationship so as to ensure animal welfare, while not being too pious or condescending.
This is equally important in day-to-day life. Being able to switch off is a must for any professional to maintain mental health, yet it’s sometimes hard to stay quiet when your friend mentions their aspiration to own 50 sausage dogs.
My question for you is, does a vet ever stop being a vet, and is a dog ever really just “a dog”?
These formulae better estimate the needs of smaller and larger patients. The flat 3ml/kg/hr underestimates for small patients and overestimates for larger patients.
This maintenance rate is in addition to rehydration rates.
So what sort of fluid should you use for maintenance?
True “maintenance” crystalloids:
used to replace ongoing fluid and electrolyte loss from normal metabolism, not to replace perfusion and hydration deficits or ongoing losses from diarrhoea, for example
sodium concentration less than plasma
potassium concentrations higher than plasma
glucose sometimes added to bring solute concentrations similar to extracellular fluid
Do you have to use maintenance crystalloids or can you use replacement crystalloids?
Replacement crystalloids are more frequently used for maintenance fluid therapy rather than maintenance crystalloids. This is because they are more readily available, we are more familiar with their use and effect, and patients are generally continued on these after perfusion and hydration deficits have been corrected.
In reality, most of the time it doesn’t really matter if we are using replacement crystalloids for maintenance therapy as the patient can manage the excess sodium, but some patients – especially cats – may require potassium supplementation. The key point is regular assessment of the patient’s hydration status and electrolytes – for example, every 12 to 24 hours for patients on IV fluids and not eating.
Many thanks to those who entered our 2022 calendar competition and sent photos of their “Perfect Pals”.
The competition is now closed, and our judges are working their way through hundreds of wonderful pictures to create a shortlist of entries, which will be published in the October issue of VN Times, with readers voting online for their favourite image.




 The process is quick – 10 to 20 seconds
The process is quick – 10 to 20 seconds


 Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.
Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.