Now that you know how to spot the signs of when a blood transfusion is needed and what blood product to administer, this article will focus on the volume of blood to give.
What PCV should I aim for?
To start us off, no real benefit exists in increasing a PCV above 30%, unless you are anticipating further losses. The reason being is oxygen delivery to tissues is optimised at that level and administering more does not add significant benefit.
How much volume to give?
There are several formulas for determining how much red blood cells are required to be given, some more simpler and less accurate than others. As a rough guide, if increasing PCV by 1, you need 2ml/kg of whole blood or 1ml/kg of packed red blood cells.
This gives me a starting volume, I administer that volume and recheck. Often, I will have to give more, but it depends greatly on the underlying disease, concurrent fluid therapy and ongoing blood losses.
How to administer?
Use a 170µm blood filter to collect any micro clots. Often, the blood is run through with a isotonic crystalloid, if so avoid administration with calcium containing crystalloid, such as Hartmann’s or lactated Ringers, as the calcium can result in activation of platelets and clots to form in the blood; so run with 0.9% saline or Plasmalyte 148.
Packed red blood cells are usually diluted with at least 100mls of 0.9% saline. The generally rule is to administer the transfusion within 4 hours and change the fluid lines after to reduce the risk of bacterial contamination. Recheck PCV and coagulation times 30 minutes post-transfusion.
How fast?
Rate of administration really depends on degree of urgency. If the patient is suffering from acute haemorrhagic shock then you can administer blood as a bolus. The risk here is acute anaphylaxis if that patient is off a different blood type or if this is not their first transfusion.
If it is not a crisis then administration should be started off slowly so monitoring for acute reactions can be performed. Start slow at 2ml/kg/hr for 15 minutes and monitor for reactions then progressively double the rate until the desired rate is reached.
Last week we covered diagnosing pancreatitis and the challenges associated with doing so. This week we look at management.
The treatment of pancreatitis largely involves supportive care and monitoring for potential complications. Here, we recap the fundamentals.
IV fluids
IV fluids are critical in the acute phase to restore perfusion to core organs and correct hydration deficits. Once achieved, the goal is then to cover maintenance requirements and ongoing losses.
Hypoproteinemia can develop due to a combination of haemodilution, increased losses in to inflammatory exudates or into gastrointestinal tract, and decreased production due to reduced intake.
Colloidal therapy or plasma can be considered, but enteral nutrition is more effective and has numerous other benefits.
Pain relief
Pain relief largely involves the use of opioids.
Pure opioid agonists, such as methadone, fentanyl constant rate infusions (CRIs) or fentanyl patches, are most commonly seen in dogs. In cats, partial agonists, such as buprenorphine, are favoured as the condition is generally less painful compared to dogs.
NSAIDs should be avoided due to concerns of poor perfusion, concurrent kidney and gastrointestinal involvement.
Antiemetic therapy
Metoclopromide CRI and maropitant are the mainstays. Antacids, such as esomeprozole, are included to help reduce the risk of gastric ulceration from stress.
Early enteral nutrition
Numerous studies have demonstrated the benefit of early enteral nutrition and patients should be encouraged to eat a low-fat diet as soon as possible. Enteral nutrition has been shown to be more beneficial than withholding food as it reduces recovery times and helps maintain enterocyte health.
If there has been a protracted period of anorexia then a nasogastric or nasoesophageal tube should be placed. A nasoesophageal tube has the added benefit of allowing excessive gastric secretions to be suctioned, as well as for feeding. Due the chronic nature of the disease in cats, oesophagostomy tubes are often placed so that nutritional support can be delivery for prolonged periods of time.
Antibiotics
Antibiotics are generally not indicated in canine pancreatitis unless markers of sepsis or if a septic exudate are found (this is an indication for exploratory surgery). In which case, triple antibiotic therapy consisting most commonly of amoxicillin, enrofloxacin and metronidazole are indicated.
It has been reported 35% of feline pancreatitis patients have bacterial infections; therefore, antibiotics are often included in the treatment of feline pancreatitis.
Exploratory laparotomy
This is indicated when the following has occurred:
Extra-hepatic biliary obstruction that does not resolve with medical management.
Septic abdomen (as mentioned above).
Pancreatic abscessation.
Prognosis
The prognosis for pancreatitis is variable and dependent on the severity of the disease.
In mild to moderate canine pancreatitis (which is the most common), the prognosis is generally good as they will normally respond well to supportive therapy and resolution of clinical signs occurs within several days of initiating treatment. However, with severe acute, necrotising pancreatitis, the prognosis is guarded as it can progress into systemic inflammatory response syndrome, disseminated intravascular coagulation and multiple organ failure – which has a high mortality rate.
The prognosis of acute feline pancreatitis is generally guarded due to the chronic nature of the disease and the propensity to involve multiple organ systems.
Although I have lots of clinical experience and have developed my diagnostic skills to a high level, at times I will be thrown a curveball, so I should never get complacent.
Figure 1. The black lymph node.
The more unusual cases are the ones I tend to enjoy most, as they really get my brain working and force me to look at every possibility – something I champion in my practice.
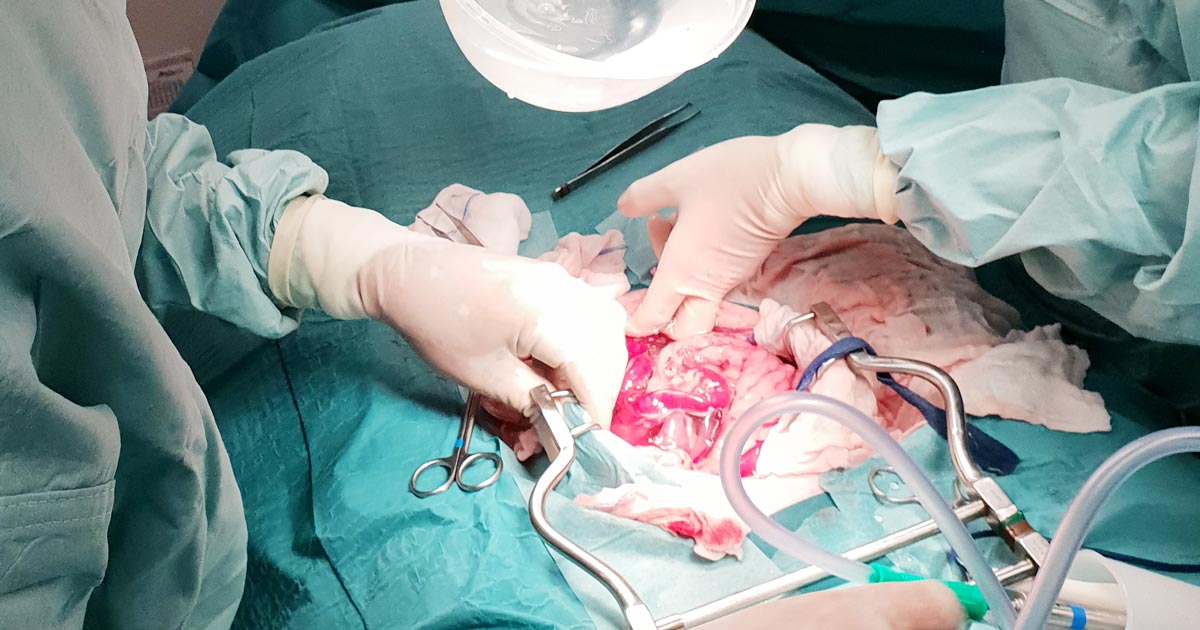
An unusual case
One particularly unusual case was of septic peritonitis – an inflammation of the peritoneal lining of the abdomen caused by a bacterial infection.
Most commonly, this is due to perforation of the gastrointestinal tract, such as a foreign body, or ulceration or from some kind of abscess often secondary to neoplasia.
Surprising findings
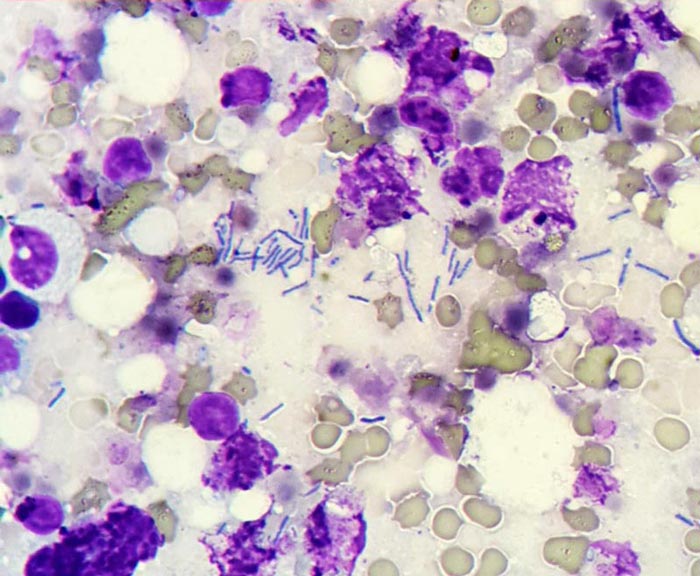
Figure 2. Detection of bacteria found after performing a fine needle aspirate.
We were unable to determine the cause of the bacterial infection in this patient via diagnostic imagery prior to exploratory laparotomy, but suspected it was due to some kind of gastrointestinal perforation due to dilated loops of hypomotile intestine.
To our surprise, the only thing we found was this black lymph node at the ileocolic junction (Figure 1).
We performed a fine needle aspirate and found bacteria under the microscope (Figure 2).
The lymph node was resected, no perforation was present, the abdomen was copiously lavaged and a Jackson-Pratt drain was placed.
This case highlighted perfectly the importance of leaving no stone unturned.
Idiopathic acute haemorrhagic diarrhoea syndrome (AHDS) – previously known as haemorrhagic gastroenteritis – remains the one disease where constant debate exists as to whether antibiotics should be used as part of the standard treatment.
The logic behind using antibiotics to prevent bacterial translocation is sound, and if AHDS is truly initiated by Clostridium species or their toxins then the use of antibiotics can be justified.
However, no knowledge exists of the true frequency of bacterial translocation in AHDS patients and conflicting evidence supports Clostridium being the initiating cause of AHDS in dogs.
Together with new data indicating the use of antibiotic therapy in aseptic AHDS patients did not change the case outcome or time to recovery, the benefit of using antibiotics must be weighed against the very real risk of selection of antibiotic resistance and other complications associated with inappropriate antibiotic use.
In this blog, we will explore the evidence against the use of antibiotics in AHDS.
Cause unknown
AHDS is characterised by an acute onset of vomiting (of less than three days’ duration) that can quickly progress to haemetamesis, and severe and malodorous haemorrhagic diarrhoea, accompanied by marked haemoconcentration that can be fatal if left untreated.
AHDS is a diagnosis of exclusion; other diseases (such as canine parvoviral enteritis, thrombocytopenia, hypoadrenocorticism, azotaemia, hepatopathy, neoplasia, intussusception, intestinal foreign body and intestinal parasitism) must be ruled out by a combination of medical history, vaccination status, complete blood count, serum biochemistry, coagulation times, diagnostic imaging and faecal testing.
Small breed dogs – in particular, the Yorkshire terrier, miniature pinscher, miniature schnauzer and Maltese – have been found to be particularly predisposed. On average, the affected dogs were young (a median of five years old).
The cause of AHDS is still unknown. Clostridium perfringens and its toxin has been incriminated as being the initiating cause; however, conflicting studies have refuted this claim. It is also difficult to determine whether overgrowth of Clostridium speciesis primary or secondary to the intestinal injury.
Virus theory
Another theory is viruses may have a role in AHDS’ aetiology. At this stage, only single agents had been investigated. It is possible a novel agent not yet been tested is the cause of this syndrome, or possibly the syndrome is the result of a very complex interaction between multiple organisms or their toxins.
For the aforementioned reason, no indication exists for the use of antibiotics to treat for the underlying cause.
Another argument behind the use of antibiotics lies in the fact most idiopathic AHDS patients have several risk factors for bacteraemia.
Necrosis of intestinal mucosa, leading to the disruption of the gastrointestinal mucosa-blood barrier; adherence of significant numbers of bacteria to the necrotic mucosal surfaces that increases the risk of bacterial translocation; significant hypoalbuminaemia indicating substantial loss of mucosal epithelial layer; splanchnic and intestinal hypoperfusion, leading to reduced intestinal barrier function; and microbial dysbiosis all contribute to an increased risk of bacterial translocation.
Although bacterial translocation has the potential to lead to sepsis, the true incidence of bacterial translocation needs to be established in idiopathic AHDS patients, as well as their influence on the outcome of the patients.
Antibiotic requirement
Use of unnecessary antibiotics not only disrupts the protective mechanisms of a normal intestinal microflora, but also the real risk of post-antibiotic salmonellosis and Clostridium difficile-associated diarrhoea.
Multiple studies have suggested antibiotics are not required in the treatment of aseptic idiopathic AHDS patients.
In a prospective study of bacteraemia in AHDS dogs by Unterer et al (2015), the incidence of bacteraemia of patients with idiopathic AHDS was 11%, compared to those of healthy controls, where it was 14%.
Transient bacterial translocation to mesenteric lymph nodes occurred in 52% of dogs undergoing elective ovariohysterectomy (Dahlinger et al, 1997), and confirmed in studies by others (Harari et al, 1993; Howe et al, 1999; Winkler et al, 2003), where portal and systemic bacteraemia was reported in clinically normal dogs.
As long as the immune system is competent, and the functional capacity of the hepatic reticuloendothelial system is not overwhelmed, the body is usually effective at eliminating organisms from the blood.
This is reflected in the Unterer et al (2015) study result, where – regardless of the bacteraemia status – all idiopathic AHDS dogs survived to discharge.
In another prospective, placebo-controlled, blind study by Unterer et al (2011), idiopathic AHDS patients were either treated with amoxicillin/clavulanic acid for six days or a placebo, and no significant difference occurred between the treatment groups concerning mortality rate, duration of hospitalisation or severity of clinical signs.
They concluded, without the evidence of sepsis, antibiotics do not appear to change the case outcome or shorten the time to recovery.
Negative impacts
The negative impacts of inappropriate antibiotic use are undeniable – especially in a time where resistance has become a worldwide public health concern.
Use of unnecessary antibiotics not only disrupts the protective mechanisms of a normal intestinal microflora, but also the real risk of post-antibiotic salmonellosis and Clostridium difficile-associated diarrhoea.
With evidence all pointing against the use of antibiotics as routine treatment of aseptic idiopathic AHDS, next time you are about to reach for antibiotics, I urge you to reconsider. Although it has taken some time to adopt and requires clear communication with clients, all vets should feel comfortable not using antibiotics for AHDS patients.
Until I started researching this Tip of The Week, I did not know the medical profession has abandoned the routine use of emesis in oral poisoning.
This is based on multiple medical literatures that have proven emesis induction does not influence the clinical severity of poisoning, the length of hospitalisation and the clinical outcome or mortality.
Although the rationale for inducing emesis is obvious, it is not necessarily evidence based. It is also dependent on satisfying a few large assumptions, all of which are untrue:
Emesis is a very effective way of removing gastric contents.
No separation exists of poison from its vehicle while inside the acidic environment of the stomach.
Poison is not absorbed through the stomach wall.
Ineffective method
Snail bait ingestions: this patient ate 500g of snail bait containing metaldehyde.
Emesis induction is an ineffective way of clearing stomach contents. A review of the effectiveness of induced emesis, with both human and canine participants, showed at 30 minutes post-ingestion of non-absorbable markers, the recovery rate averaged between 17.5% and 52.1%, but never exceeded 62%.
In fasted puppies, this was even lower at 2% to 31%, despite inducing emesis immediately after marker administration. These have been confirmed by the presence of poisonous materials in the stomach of dead patients, despite effective emesis induction until clear fluid was brought up.
The clinical outcome only improves if the systemic exposure of a toxicant is reduced by more than half. However, considering animals rarely practice restraint, the ingested amount is unlikely to be exactly the lethal dose and no more. Therefore, even reducing the ingested toxic dose by 62% is unlikely to make a clinical difference.
Furthermore, most patients rarely present within 30 minutes of ingesting a toxicant, thus further reducing its efficiency.
The absorption conundrum
Some may argue the retrieval of metaldehyde or anticoagulant rodenticide granules from vomitus is indicative of reducing the toxicant dose. This could be true, but only if emesis was induced immediately after ingesting the poison.
The poison itself is colourless and has a different absorption characteristic to the coloured vehicle (granule); therefore, the presence of granule only serves to confirm ingestion, but is of no indication whether the poison has already been absorbed.
Contraindications
Many well-recognised absolute contraindications also exist to inducing vomiting:
Ingestion of oils, which includes waxes that melt to oil in the internal body environment, as this poses a high risk of lipoid and bacterial pneumonia. This is of significant veterinary significance, as wax is routinely used in rodenticide baits.
Ingestion of hydrocarbons and other volatile substances, or caustic or corrosive substances.
When the mental status is altered – for example, hyperexcitable or depressed mental state.
Where the patient is at risk of seizures (seizures can be induced by emesis).
Increased intracranial pressure.
Risk of intracranial or cerebral haemorrhage – for example, thrombocytopenia or abnormal clotting parameters.
Other less severe, yet important, reasons include:
delays administration of more effective treatment, such as activated charcoal, antidote or other treatments
risk of aspiration pneumonia
hypochloraemia in recurrent emetic patients
significant CNS and respiratory depression from apomorphine
rare, but reported, complications such as cerebral haemorrhage, oesophageal tear/ rupture, hiatal hernia, gastric rupture, pneumothorax and pneumomediastinum
legal implications – for example, if the product information clearly states emesis should not be induced
A place for everything
Emesis induction is not a benign procedure. It still has its place in certain circumstances, but its use in the routine management of oral poisonings may need to be reconsidered – especially if it means delaying administration of a more effective treatment, such as activated charcoal.
So, after all this, how do I tackle this information? It is a bit hard to swallow. My clinical experience is emesis is generally safe, especially in canine patients using apomorphine. So, I still feel some merit exists in reducing the amount of toxicant in the stomach if you have a chance – and in some situations, you don’t know until you try.
Emesis after ingestion of a toxic dose of chocolate can be incredibly rewarding, even six hours after ingestion, leading to patients not developing clinical signs at all.
Overall, I am biased by my personal successes with emesis, so still feel a time and place exist for emesis induction. But I now stop and question my decision to induce emesis, whereas I did not hesitate before.
Many clients have difficulty persuading their cat to take tablets. Image source unknown.
OK, a potentially controversial one this…
There is a lot of evidence highlighting resistance to antibiotic therapy both in the human and veterinary fields. My understanding is that this is, in part, due to poor compliance.
I’ve certainly come across clients who have difficulty giving tablets to their cat, and have also seen cases that “appear” to respond poorly to amoxicillin/calvulanic acid but then respond rapidly to Convenia.
So, my argument is that injecting a long-acting preparation licensed for the treatment of soft tissue infections in cats (having bactericidal activity to the “usual suspect” oral bacterial flora of the cat) is preferable to giving oral meds that owners find difficult, and in some cases impossible, to administer.
I might even suggest this may result in less resistance.
 To start us off, no real benefit exists in increasing a PCV above 30%, unless you are anticipating further losses. The reason being is oxygen delivery to tissues is optimised at that level and administering more does not add significant benefit.
To start us off, no real benefit exists in increasing a PCV above 30%, unless you are anticipating further losses. The reason being is oxygen delivery to tissues is optimised at that level and administering more does not add significant benefit.