The PCV and total solids (TS) test is simple, yet informative – but is often misinterpreted or underused.
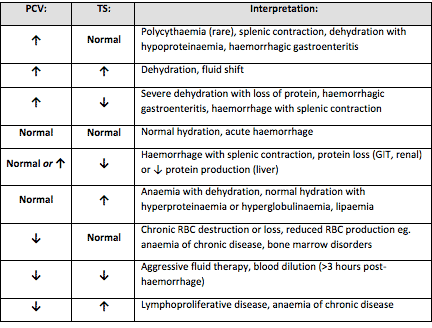
Table 1. Changes that can be found on a PCV/TS and possible causes (click to zoom).
It is important to remember all test results need to be interpreted in light of the patient’s history, presenting clinical signs and general physical examination findings.
The various changes that can be found on a PCV/TS, and the possible causes, are detailed in Table 1. Many of the differentials can be included or excluded based on the history, clinical signs and examination findings.
Misconceptions
I would like to highlight some common misconceptions I find with PCV/TS interpretation.
A normal PCV/TS means the patient cannot be dehydrated
The concept all dehydrated patients will have an elevated PCV/TS is inaccurate. Patients will have to be severely dehydrated to see an elevation in both PCV/TS.
Dehydration should be based primarily on physical examination findings, not based primarily on PCV/TS results.
A patient with a normal PCV could not have lost blood as the PCV should be low
Patients can have acute whole blood loss, which is not reflected in the PCV at presentation. This could have been caused by a number of reasons – for example:
the extravascular fluid has not yet shifted down the hydrostatic pressure gradients
the patient has not ingested water since the time of blood loss
IV fluid has not been given to correct the hypovolaemia
Once the fluid shifts, the patient drinks water or IV fluids are administered, the PCV/TS will drop due to haemodilution.
An elevated PCV means the patient is dehydrated
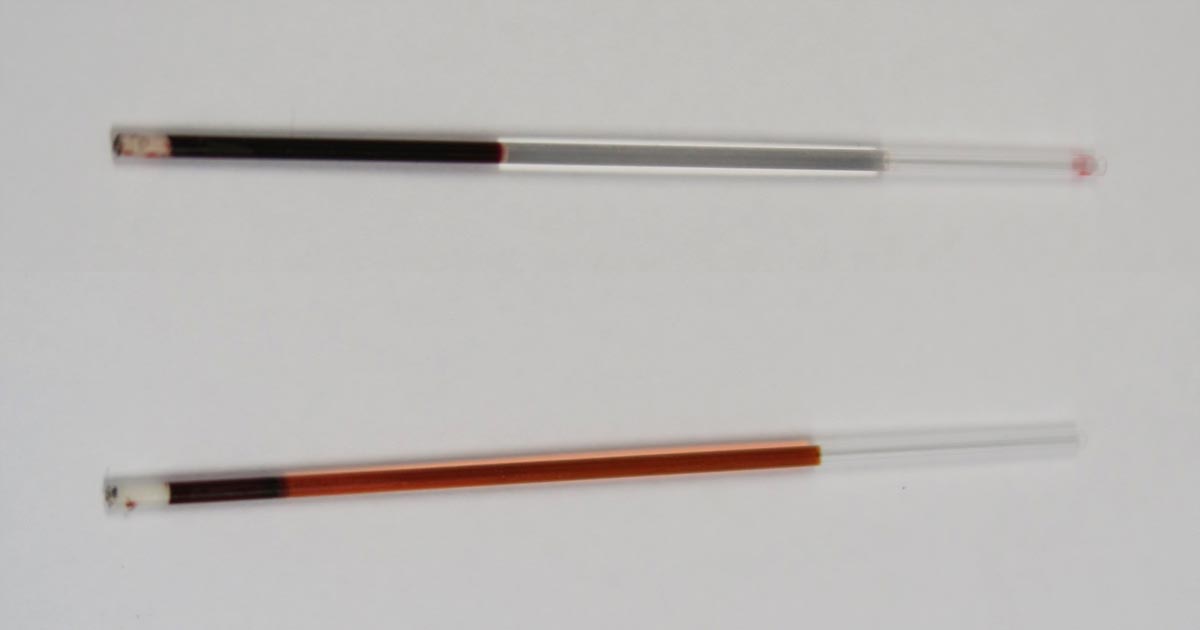
PCV tubes.
This is probably the most common change I see in my patients – and it is not because they are all dehydrated.
The most common cause of this change is stress-induced splenic contraction. The spleen stores red blood cells. Under the influence of adrenalin, the smooth muscle in the spleen contracts and the stored red blood cells are pushed into circulation.
The next most common cause would be haemorrhagic gastroenteritis, where a fluid shift into the gastrointestinal tract has occurred.
Assessment of the serum colour can also provide valuable information. White or lipaemic serum can cause artifactually high TS. Haemolysed serum with a low PCV can indicate a haemolytic anaemia.
Next time you perform a PCV/TS, look at Table 1 and consider the other differentials for your results.
Postoperatively, gastric dilatation-volvulus (GDV) patients remain in our intensive care unit for at least two to three days.
Monitoring includes standard general physical examination parameters, invasive arterial blood pressures, ECG, urine output via urinary catheter and pain scoring.
I repeat PCV/total protein, lactate, blood gas and activated clotting times (ACT) immediately postoperatively and then every 8-12 hours, depending on abnormalities and patient progress.
Patient recovering in the pet intensive care unit. As well as standard monitoring parameters, GDV patients have constant ECG, arterial blood pressure and urine output monitoring to enable the early detection and correction of abnormalities.
I always repeat these blood tests postoperatively, as IV fluids given during the resuscitation and intraoperative period often cause derangements. I use the results to guide my fluid therapy, but also take it with a grain of salt.
IV fluids
I generally continue a balanced and buffered crystalloid. The rate depends on blood pressures, urine output and assessment of general physical examination parameters for perfusion and hydration, but I try to avoid fluid overload and reduce the IV fluids postoperatively as soon as possible.
Coagulopathy
Prolonged clotting times are frequently seen as a result of consumption in a dog with GDV. However, one should note it can also occur as the result of haemodilution.
As the underlying disease process has been corrected, and haemostasis achieved during surgery, I usually monitor ACTs, but may not necessarily treat with blood products as prolonged ACTs do not always translate to clinical bleeding. Unless clinical evidence of bleeding exists, I generally hold off treatment and monitor.
Hypoproteinaemia
Low total protein is also common. This is generally due to haemodilution from fluid resuscitation. However, a low total protein does not mean oedema will develop, or that it requires management. I generally track the protein levels, use conservative fluid therapy and try to correct it by instituting enteral nutrition as soon as possible.
Electrolyte imbalances
Hypokalaemia is a common complication of fluid therapy. This can be rectified with potassium supplementation in the IV fluids.
Hyperlactataemia
If present post-surgery, this is usually corrected with a fluid bolus. However, I always assess for other things that may affect oxygen delivery to the tissues, such as poor cardiac output (arrthymias), hypoxaemia (respiratory disease) and anaemia (from surgical blood loss).
Arrhythmias
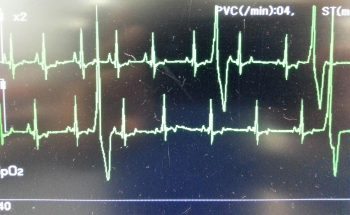
Ventricular arrhythmias are common post-surgery. Accelerated idioventricular rhythms are the most common cause, especially if a splenectomy was performed.
Ventricular premature contractions are common postoperative arrhythmia.
Before reaching for anti-arrythmia medications, first check and correct:
electrolyte abnormalities
hypoxaemia
pain control
hypovolaemia or hypotension
If they are still present, despite correction of the above, consider treating the rhythm if:
multifocal beats (ventricular premature contractions of various sizes)
overall rate greater than 190 beats per minute
R-on-T phenomenon
low blood pressure during a run of ventricular premature contractions
I start with a bolus 2mg/kg lidocaine IV and start a constant-rate infusion of 50ug/kg/min to 75ug/kg/min.
Anaemia
It is common to have a mild anaemia post-surgery, due to a combination of blood loss and haemodilution. In the absence of transfusion triggers – such as increased heart rate, increased respiratory rate or hyperlactataemia – it does not require treatment.
Vomiting
Anti-emetics are the first line of medication. Non-prokinetic anti-emetics, such as maropitant and ondansetron, can be used immediately; otherwise, after 12 hours, metoclopramide can also be used postoperatively. If the patient remains nauseous despite these medications, the placement of a nasogastric tube can ease nausea by removing static gastric fluid.
Excessive pain relief may also contribute to the nauseous state.
Pain relief
I mostly rely on potent-pure opioid agonists, such as fentanyl constant-rate infusions and patches. This is generally sufficient for most patients. Ketamine is occasionally used.
Some drugs listed in this article are used under the cascade.
Now we cover the three things you need to do as soon as a suspected case is presented:
IV fluid resuscitation
decompression of the stomach
pain relief
Depending on the number of staff you have, all of these can be performed simultaneously. If not, follow the above order as shock is the most imminent problem.
Catheter placement
Fluid resuscitation is relatively straightforward. Most GDV patients will be in some degree of shock, varying from mild to severe. Regardless of the actual degree, all patients will require IV fluids.
The placement of IV catheters is particularly important; their numbers and diameter will influence the rate of response to treatment. Large-bore catheters allow faster flow of fluids compared to smaller ones, while multiple catheters allow concurrent delivery of two bags of fluids as opposed to one – particularly important in large dogs. Therefore, always try to place the largest catheter possible (for example, 18G or larger for large-breed dogs) into the cephalic veins.
Once the catheters have been placed, collect 2ml to 3ml of blood for baseline measurements. These can be collected directly from the catheters and should include:
PCV/total protein
blood gas analysis
lactate
activated clotting time
electrolytes
later, full haematological and biochemical analysis
Once the baseline bloods have been collected, fluid resuscitation should start immediately.
How much, how fast?
Fluid resuscitation is relatively straightforward, says vet Gerardo Poli.
How much fluid should you deliver, and how fast? My “go to” fluid is crystalloids and I generally start with a 20ml/kg bolus of an alkalinising crystalloid.
I perform bolus therapy, so 10ml/kg to 20ml/kg fluid doses rather than shock rates 90ml/kg/hr, as I feel it allows me to better titrate my fluid therapy to effect. It also helps minimise excessive fluid administration and the problems with haemodilution – such as anaemia, hypoproteinaemia and prolonged coagulation times.
As fluids are being delivered, I administer pain relief and start gastric decompression (covered next week).
The decision to administer more fluids depends on whether I have achieved some end point resuscitation variables, such as:
a reduction in heart rate
a reduction in capillary refill time
an improvement of mucus membrane colour
improvement in pulse pressures
Improvement in mentation is not often reliable as the sedative effect of analgesia, which I generally give during fluid resuscitation, often confounds this effect.
Shock therapy
If evidence of shock still exists, despite the initial fluid boluses and gastric decompression, I will consider more fluids. This can include hypertonic saline or colloids.
In my experience, a repeat of a smaller dose of crystalloid fluid bolus is often adequate (10ml/kg). The transition on to hypertonic saline (7% solution) or colloids is influenced by the results of the aforementioned baseline diagnostics.
A reduction in PCV/total protein suggests blood loss. In this case, I will consider either hypertonic saline (3ml/kg to 5ml/kg of 7% solution), a dose of colloids or even blood products, such as whole blood or packed red blood cells.
If significant prolongation in activated clotting time occurs, likely from consumption, then I may incorporate fresh frozen plasma into my fluid therapy. This is in anticipation of possible surgery, where prolonged coagulation times can not only be troublesome, but life-threatening.
Lactate
A quick note on lactate – I don’t use the baseline reading as a prognostic indicator or an indicator of gastric necrosis. This is supported by recent findings claiming it is not the level of lactate that is predictive, but the degree of improvement in response to fluid resuscitation and gastric decompression.
I have seen unreadable lactate levels – greater than 15mmol/L – in patients who returned to reasonably normal levels within an hour of stabilising. These patients also went on to survive surgery.
Pain relief
After starting IV fluid resuscitation, I generally administer pain relief while the team is preparing for gastric decompression. To keep things simple, I stick to an easily accessible pure opioid agonist at 0.2mg/kg IV. I avoid subcutaneous or even intramuscular administration as the patient is often in shock; the peripheral blood is shunted centrally to the heart and the brain and absorption can be variable.
I find this offers a reliable and great degree of pain relief that helps reduce anxiety levels and, consequently, reduces oxygen demand. It has minimal cardiovascular effects and the mild sedative effect also helps with the process of decompression.
Christmas can be a busy time for vet clinics, so here is a list of common intoxications and conditions to keep an eye out on during the festive period.
Chocolate
Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.
I always perform emesis in patients that have ingested chocolate, even hours after ingestion as often large amounts can reside in the stomach.
Remember that cardiac arrhythmias can also occur in clinically normal looking patients, so perform an ECG.
The toxic components can be reabsorbed through the bladder wall; therefore, urinary catheterisation is a part of management of this intoxication.
Onions
Onions used in roasts and on BBQ’s can cause Heinz body formation, haemolytic anaemias and pigmenturia.
This is not a common intoxication, but should be considered in anaemia patients and those with discoloured urine.
Raisins
Commonly used in Christmas cakes and puddings. They can cause acute kidney failure, the exact mechanism of action is unknown, and there does not appear to be a dose-dependent relationship.
It should always be a differential for azotemic patients this time of year.
IV fluid induced diuresis for 48 hours is the safest way to manage raisin exposure.
Mistletoe
The berries can be fatal, even if only a couple are ingested.
Ethylene glycol
In colder climates, ethylene glycol can be a very common toxicity.
This sweet liquid is very attractive to pets and can cause acute renal failure, with the first signs being acute onset ataxia.
Macadamia nuts
Macadamia nuts are common in some parts of the world. They result in joint pain in the hocks and carpus leading to weakness and ataxia.
Often confused with trauma and soft tissue injuries. Hyperextension of the hocks and sometimes flexion of the carpus are the clinical features.
Xylitol
Xylitol is a sugar-free product used in lollies and baking.
In dogs, it triggers endogenous insulin to be released and a subsequent hypoglycemia develops. It can also cause hepatic failure.
As a general rule, I approach all intoxications as if they could be fatal as it is rare to know exactly how much of the toxic agent they have been exposed to. I consider if a patient I am treating for intoxication never develops clinical signs and wonder whether it was going to or not is the best outcome.
Strings
Look under the tongue.
Linear foreign bodies can be difficult to diagnose. Some features on abdominal radiographs to look out for include abnormal bunching of the small intestines, and “c” and “comma” shaped gas patterns.
Christmas meals
Gastroenteritis is the most common presenting condition over the Christmas period, with dietary change and indiscretion often being the culprit.
Bones can lead to obstructions from oral cavity to the intestines and can also cause constipation.
Leftover meat trimmings, often fat laden, are a common cause of pancreatitis.
BBQ skewers
In some parts of the world (Australia especially) BBQs are common around Christmas time.
BBQ skewers can cause gastrointestinal tract perforation and septic peritonitis.
Because they are not radiopaque they are often difficult to diagnose.
Pulse oximetry is a very useful diagnostic and monitoring tool that has become commonplace in veterinary clinics. It measures the percentage of haemoglobin saturated with oxygen, and is an indirect measure of arterial oxygen levels.
Dog with pulse oximetry.
However, here are several important points to help you understand the limitations of pulse oximetry.
Causes for false readings
Falsely low readings:
motion artefact
peripheral vasoconstriction/low tissue perfusion from hypothermia or shock
pigmentation of mucous membranes
thick hair coat
Falsely high readings:
haemoglobin abnormalities (carboxyhaemoglobin and methaemoglobin, for example)
False sense of security
Pulse oximetry can give us a false sense of security. We hold on to the adage “95% and above means everything is going along swimmingly”, but that couldn’t be further from the truth:
Pulse oximetry can give us a false sense of security.
It does not detect hypoventilation or apnoea: it can take several minutes for apnoea to result in hypoxaemia that is detected on pulse oximetry; therefore, it cannot be used as a sole measure of respiratory adequacy. This is best measured by capnography.
A common misconception is the oxygen saturation will drop with patients with anaemia. This is incorrect. The haemoglobin present in the decreased number of red blood cells will still be saturated to normal levels. However, this cannot be interpreted as the patient having adequate oxygen delivery to its tissues.
One last point: due to the oxyhaemoglobin dissociation curve, any drop below 94-95% is significant and warrants investigation. At 95% SpO2 the partial pressure of oxygen in the arterial blood is 80mmHg (normal), but at 90% SpO2 the partial pressure is 60mmHg (severe hypoxaemia) – for only a small percentage decrease, there is an exponential reduction in arterial oxygen content. This is even more important when patients are receiving oxygen therapy as the patient’s SpO2 should be 99-100% normally. So when a patient has an SpO2 of 95%, but is on high rates of oxygen, then significant respiratory compromise/disease must be present for an SpO2 of 95% or lower to occur.
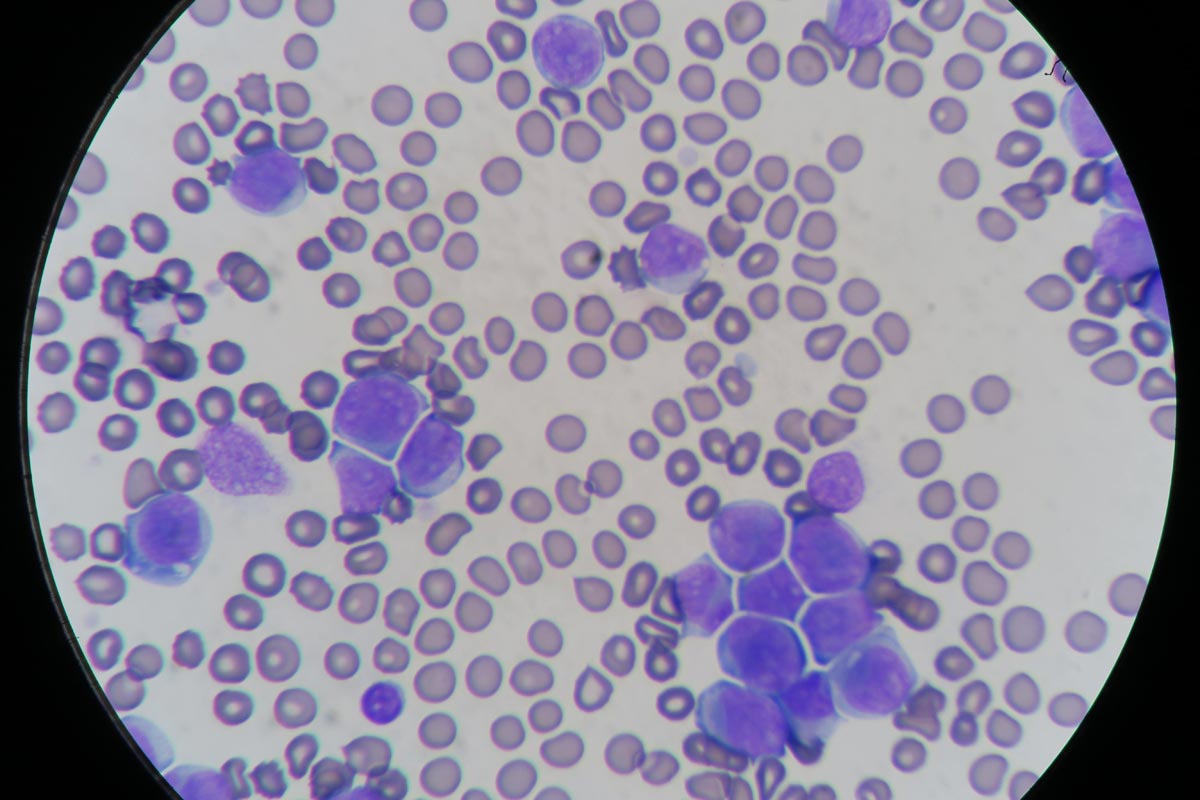
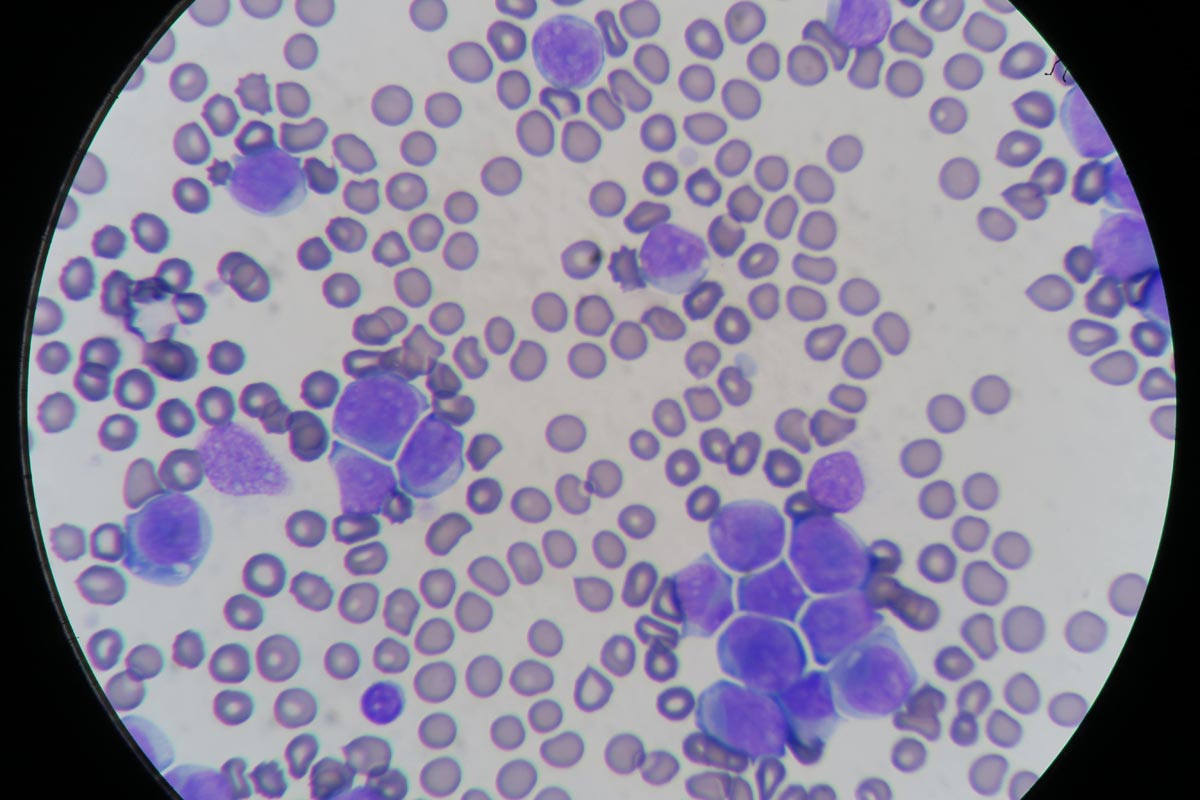
Blood smear evaluation is an often overlooked, but very important, aspect of an in-house haematology.
With the advancement in haematology analysers that can now detect reticulocytes and even band neutrophils, some practitioners are beginning to rely solely on the numerical data alone in evaluating the patient’s blood.
Patient with elevated white blood cells caused by leukaemia (click to zoom).
The art of blood smear interpretation is on the decline. However, it is an extremely valuable skill that must be practised and perfected and really should be part of every in-house haematology.
Plus points
What are the benefits of being good at blood smears?
Identifying a regenerative response, looking for reticulocytes (polychromatophils).
Looking for other possible causes of an anaemia – such as Heinz bodies, infectious microorganisms or spherocytes, which can indicate an immune-mediated haemolytic anaemia.
Confirming thrombocytopenias, as frequently platelet clumping can be reported as a thrombocytopenia.
Assessment of the nature of a leukocytosis. High leukocyte counts do not always mean infection. Neutrophilia can be caused by both elevated immature and mature neutrophils. Determining the nature of neutrophilia can provide crucial information in identifying the underlying cause and if the patient is coping or not. Apart from infection, other causes can include stress, corticosteroids and neoplastic leukaemias.
Normal leukocyte counts do not always mean the patient is okay. Patients can have severe left shifts, but normal leukocyte counts.
Practice makes perfect
Blood smear evaluation begins with becoming accomplished at producing great diagnostic smears. This takes practice; poorly performed smears can be non-diagnostic and frustrating to assess for both yourself and an external pathologist.
A few tips on the technique:
Use a very small drop of blood. If you have picked up too much blood with the “spreader” slide, lift off and start the smear away from that drop of blood.
Angle the “spreader” slide about 30°. The bigger the angle, the shorter your smear.
Push the “spreader” slide forward.
The smear should end at about half to three-quarters of the way down the slide and must have a “feathered edge”.
While hyperadrenocorticism is not an uncommon incidental finding in patients presenting to our emergency clinic, hypoadrenocorticism is a lot less common. Or, possibly, more frequently underdiagnosed.
Textbook clinical presentations combined with haematology and biochemicial changes can make diagnosis straightforward, but not all patients will present with all the classic signs.
The SNAP cortisol test is a quantitative ELISA test that measures the level of serum cortisol in dogs.
To complicate things further, hypoadrenocorticism is the great mimicker of diseases; it is often impossible to arrive at a definitive diagnosis without knowing the cortisol levels.
The SNAP cortisol test allows clinicians to determine cortisol levels in-house – a blessing to those of us who work out-of-hours – but is not without its limitations.
Suspicious signs
Patients with hypoadrenocorticism often present with vague and non-specific clinical signs, but certain clinicopathological changes help raise the suspicion:
a decrease in sodium-to-potassium ratio (below 1:27)
azotaemia
an inappropriately low urinary specific gravity, despite evidence of dehydration or hypovolaemia
a leukogram unfitting to the degree of illness of the patient (a “reverse stress leukogram”- neutropenia, lymphocytosis, eosinophilia)
anaemia
hypoglycaemia
hypercalcaemia
Although most Addisonian patients will not present with all these signs – especially those in the early stages of disease or those with atypical Addisonian disease (glucocorticoid insufficiency only) – any patients showing any of these haematology and biochemicial changes should have hypoadrenocorticism ruled out as part of the diagnostic plan.
Imperfect ELISA
The SNAP cortisol test has been advertised as an in-house assay to aid the diagnosis, treatment and management of both hyperadrenocorticism and hypoadrenocorticism, although the quality of the result is not perfect. This quantitative ELISA test measures the level of serum cortisol in dogs.
In one study1, the SNAP cortisol test appears to have a good correlation with an external laboratory chemiluminescent assay test; however, in 12.8% of cases (5 of 39 patients), the SNAP test result could have led to a different clinical decision regarding the management of the patient.
Since long-term Cushing’s management relies on reliable, repeatable cortisol level detection, this high level of discrepancy is unacceptable, especially when more accurate alternatives are available at external laboratories.
Still useful
Despite this, it is still very useful helping to assess for the presence or absence of hypoadrenocorticism, especially in an emergency setting.
I use the SNAP cortisol to measure the resting cortisol level. If it is below 2ug/dL or in inconclusive range (between 2ug/L and 6ug/L), but the clinical picture suggests hypoadrenocorticism, I would perform an adrenocorticotropic hormone (ACTH) stimulation test and send samples to an external laboratory. If it is well above the inconclusive range, I would not perform an ACTH stimulation test.
In summary, I think the SNAP cortisol test can be useful in helping assess for hypoadrenocorticism, but would still recommend performing an ACTH stimulation test and running the samples externally.
However, use it with caution for hyperadrenocorticism diagnosis and its long-term management – especially when more accurate and economical alternatives are available.
The past decade has seen a significant shift in the prevalence of both FeLV and FIV in most European countries. This, coupled with a better understanding of the viral dynamics of FeLV, will influence the interpretation of the results of in-house diagnostics tests of these viral infections.
FeLV is an RNA virus that undergoes classic retroviral replication that incorporates its own genes into the host genome, known as provirus. Of those infected, approximately 30% to 40% will not be able to mount an effective immune response and will become persistently viraemic (“progressors”).
The SNAP FeLV antigen/FIV antibody test.
These cats will have a high proviral load, remain persistently antigen-positive and eventually succumb to the disease. These cats have a poor prognosis, with 70% to 90% succumbing to the disease within 18 to 36 months.
The remaining infected cats will become “regressors”. These cats will be able to mount an effective immune response and, eventually, become antigen-negative; however, will still be provirus-positive as these cannot be completely eliminated.
In extremely unusual circumstances, these cats may recrudesce and become viraemic again later in life – previously known as “latent” infection – but these cases are extremely rare. Cancer and corticosteroid-induced immunosuppression is thought to be responsible in these cases.
FeLV prevalence
The prevalence of FeLV is now much lower compared to 10 to 15 years ago, with successful culling and selective breeding programmes meaning the risk of false positive results is increased.
A positive result could be because it is a true positive (FeLV-associated disease), transient positive or false positive. A much higher chance exists of a true positive within at-risk groups – young cats with lymphoma, anaemia or leukopenia, and cats with unusual infection or unexplained wasting diseases.
A positive result in healthy cats should be considered suspicious. These cats could be regressors and should be retested 12 weeks later, where the result should become negative. Alternatively, it could be a false positive and an external lab should be used to confirm infection, preferably using an alternative method – such as DNA PCR – to test for the presence of provirus.
FIV prevalence
The interpretation of FIV test results, both in light of new disease prevalence data as well as epidemiological evidence, needs to be revised.
The prevalence of FIV in Australia is a lot higher than previously thought. In a study based on cats from the inner Sydney area, the prevalence of FIV is 16% in domestic cats with outdoor access, 21% to 25% in two feral cat colonies and up to 32% among some populations of “sick” cats (Norris et al, 2007). An owner survey revealed almost 80% of Australian cats spend some time outdoors, posing most cats at a high risk of FIV exposure.
Although no current statistics exist on the percentage of cats vaccinated for FIV, an increased vaccination rate will have a significant impact on the reliability on the results from in-house tests.
Combination test
As the name suggests, the SNAP combination FeLV antigen/FIV antibody test detects the presence of FIV antibodies. This test cannot distinguish antibodies from those naturally infected, vaccinated or derived from maternal antibody. To add to the confusion, antibodies can take anywhere between two to four weeks – and sometimes up to six months – to develop after initial infection.
To overcome this problem, PCR is needed to determine the presence of viral RNA (ELISA-positive, PCR-negative).
It should be noted the presence of FIV antibodies in naturally infected individuals is only indicative of a persistent infection. It is not correlated with the presence of immunodeficiency or diseases directly related to FIV. In fact, new epidemiological evidence shows FIV infection does not cause illness in most cats and does not seem to cause reduced lifespans.
Summary
Any cat having a FeLV-positive SNAP test result is considered to be actively shedding virus, regardless of its health status. A cat that has a FeLV-negative SNAP test means it is not viraemic, thus not shedding virus, but does not necessarily mean it is free from infection.
On the other hand, the true FIV status of a cat remains difficult to determine in-house. A positive result could mean persistently infected, maternal antibody, vaccine-induced antibody or a false positive, whereas a negative result could mean true negative, early infection or false negative.
Regardless of the result, the true relevance of the FIV status in the acute management of an otherwise healthy cat is questionable, considering the new epidemiological findings.






 Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.
Numerous online calculators can determine whether a toxic dose has been consumed and they are a great place to start.