Although I have lots of clinical experience and have developed my diagnostic skills to a high level, at times I will be thrown a curveball, so I should never get complacent.
Figure 1. The black lymph node.
The more unusual cases are the ones I tend to enjoy most, as they really get my brain working and force me to look at every possibility – something I champion in my practice.
An unusual case
One particularly unusual case was of septic peritonitis – an inflammation of the peritoneal lining of the abdomen caused by a bacterial infection.
Most commonly, this is due to perforation of the gastrointestinal tract, such as a foreign body, or ulceration or from some kind of abscess often secondary to neoplasia.
Surprising findings
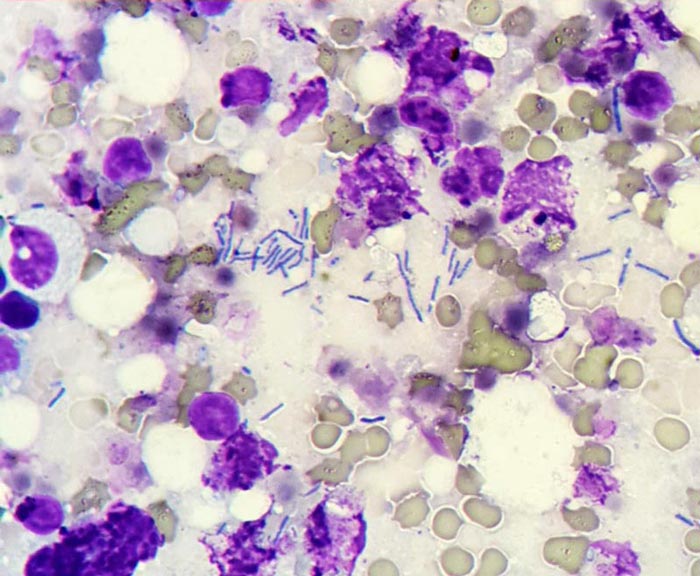
Figure 2. Detection of bacteria found after performing a fine needle aspirate.
We were unable to determine the cause of the bacterial infection in this patient via diagnostic imagery prior to exploratory laparotomy, but suspected it was due to some kind of gastrointestinal perforation due to dilated loops of hypomotile intestine.
To our surprise, the only thing we found was this black lymph node at the ileocolic junction (Figure 1).
We performed a fine needle aspirate and found bacteria under the microscope (Figure 2).
The lymph node was resected, no perforation was present, the abdomen was copiously lavaged and a Jackson-Pratt drain was placed.
This case highlighted perfectly the importance of leaving no stone unturned.
Abdominal ultrasound is an invaluable diagnostic tool that can give us far more information about abdominal organs than radiographs. It can also be a very daunting procedure – especially for clinicians unfamiliar with how the machine operates.
One of the biggest frustrations with using the ultrasound machine stems from not knowing what each button is for, or how to use them to adjust the image quality appropriately, to obtain the information required.
Over the next few posts, I will offer you hints and tips on how to get started. Once you understand what all those buttons and dials are for, you should be able to operate just about any ultrasound machine with confidence.
I will also explain how to perform an abdominal ultrasound in a systematic manner, as well as how to get the most information out of it.
Buttons and their uses
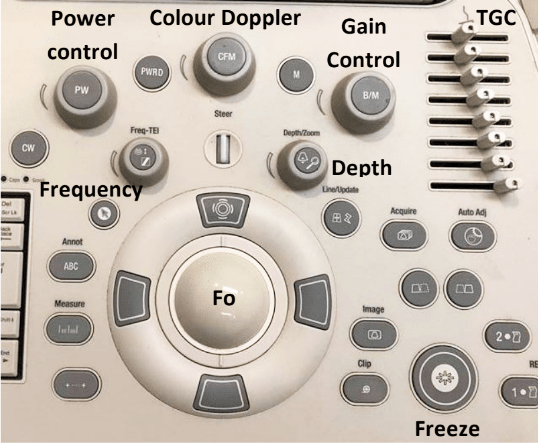
Figure 1. An ultrasound machine control panel.
Figure 1 is an example of a typical ultrasound machine control panel. The following explains the different buttons and dials present, and their uses.
Power control
The power or output control affects the strength of the emitted sound pulse. Keep this to as low as possible for the required depth.
Gain control
The gain control regulates amplification of all returning echoes non-selectively – that is, it makes the entire image brighter.
Time gain compensation
The time gain compensation (TGC) selectively regulates amplification of echoes returning from various depths.
The objective of TGC is to provide a uniform image from top to bottom. Returning near-field echoes are already strong and may actually need to be suppressed. Far-field echoes are weaker and, therefore, may need to be amplified more according to the depth from which they return.
Depth
The depth allows you to choose how deeply into the tissues the image will display. Use an appropriate depth to view the structure of interest – that is, adjust the depth so the structure fills three-quarters of the field of view.
Focus
The focus (Fo) provides the best image at a certain depth and should be adjusted so it is at – or just behind – the area of interest. The focal point is the yellow arrow on the right side of the screen, which can be moved up and down with the Fo tracking ball.
Freeze
The freeze-frame control creates a frozen on-screen image for closer inspection, annotation, measurements using electronic calipers and producing permanent documentation with digital, film or paper images.
Clip
The clip button records a short video clip.
Colour Doppler
The colour Doppler assesses fluid flow. It is useful for differentiating between a vessel and structure of equal echogenicity, such as an adrenal gland or lymph node, and for determining the vascularity of a structure, such as a torsed spleen, mass lesion or abscess.
Flow towards the transducer = red, while flow away from the transducer = blue.
Cat bite abscesses are one of the most common presentations in general practice.
Even in an emergency setting, I see a number of these patients. Usually they are obvious, but, occasionally, they’re not so obvious and the patient comes in lethargic, inappetant and often “painful”.
Overly dramatic?
One thing I’ve learned in my time is a cat bite abscess should be considered for all cats that have pyrexia. For a pyrexic outdoor cat without an obvious cause, I include a whole body clip as part of my diagnostic process. This is because a cat bite can start as a cellulitis and bite wounds are very small.
Whole body clipping may sound dramatic, but it has saved me many times and helped rule out cat bites as a major differential for cats with pyrexia.
Standard approach
Everybody treats cat bite abscesses in their own way, but here’s my approach:
Any warm, painful area or swelling should be clipped to look for bite wounds.
I always look for all four tooth marks – you can miss wounds and other developing abscesses by focusing only on the obvious bite wounds.
You must establish drainage, surgically explore and lavage. This means patients are always placed under heavy sedation or a full anaesthetic. Why do I always recommend this? I have found cat nails, hair and teeth in abscesses before; without removing those foreign bodies, the abscess won’t heal and antibiotics won’t be effective.
I almost always administer antibiotics, even if I have removed an abscess en bloc and no contamination exists.
Pain relief is always indicated, depending on the age and stability of the patient. An NSAID is my preference, but only after I have corrected my patient’s fluid deficits, otherwise I select a different type of analgesic.
Drains? Sometimes I place drains in very large abscesses, but mostly I prefer to close primarily after appropriate debridement.
At the end of January I travelled down to Nottingham for the third annual Student Equine Veterinary Association (SEVA) symposium.
Image: Roman Milert / Fotolia.
The weekend was crammed with lectures, practicals and seminars relevant to horses in particular, for equine enthusiasts from all UK vet schools – and even some from further afield.
Auspicious start
Any congregation of vet students is eventful, and the weekend kicked off with us accidentally setting the toaster on fire before making our way to campus for the first set of lectures.
It’s always interesting to see other vet schools in their settings: the short journey through the Midlands countryside was quite different from our commute in the West End of Glasgow.
Sarcoid legend
Big names in the equine vet world were present to deliver talks on a range of subjects from the emergency colic, orthopaedics, the racing vet and reproduction.
The British weather was against some of the guest speakers and, after battling the snow to make his plane, Prof Derek Knottenbelt arrived a little later than planned to deliver his lecture on oncology – a highly amusing and informative presentation that proved the renowned sarcoid legend was worth the wait.
Jonathon Pycock, as well as delivering a talk on reproduction, ran a seminar on the Veterinary Defence Society (VDS) and through the medium of hilarious anecdotes, encouraged students to make use of the VDS in the future should they ever get into a sticky legal situation.
Practicals covered a wide range of subjects, but I had chosen cardiology and farriery.
Matters of the heart
The cardiology practical covered auscultation of the normal horse and localisation of a heart murmur in the abnormal horse, followed by ultrasound scanning of the heart; something I’d never done before.
We were able to use electronic stethoscopes during the session – the difference they made was incredible (shame I haven’t got a spare £400 to upgrade from the manual one). We then had a related seminar on diagnosing and interpreting heart murmurs from auscultation recordings and ultrasound videos, which was very helpful in trying to distinguish heart sounds more clearly.
Veterinary students taking part in the cardiology practical.
Local Army Farriers ran a session on farriery, allowing us to practice removing a shoe, putting a shoe on and the approach to an abscess in the foot. We later discussed the use of different remedial shoes for various conditions and urged us to communicate effectively with farriers in order to work together to achieve the best solution to problems of the foot.
Party on
Saturday evening played host to a black tie ball, with great food and wine and a live string band, before continuing the party with many of the speakers also dancing among the students until the early hours.
As with all vet events, I had a fantastic time and would urge other students to go to at least one of these symposiums or congress during their time at vet school.
Even if it’s revision, I find learning something you think you might know reasonably well in a different format will highlight areas you need to work on and help consolidate things better. While the focus is primarily academic, I think these weekends are still always true to the vet school mantra of “work hard, play hard”, and I always have a fab time.