A bleeding patient can be overwhelming but there are only a few pieces of equipment that you need and a step-by-step approach.
1. Ask yourself the question:
“Is my patient bleeding due to local issue (trauma, for example) or from a system coagulopathy?”
If a local issue is suspected like trauma, then treat as required. If unsure, treat the trauma anyway and then put your Sherlock Holmes hat on and let’s get started…
2. Assess the history
Important history questions:
Recent trauma?
This will help determine of the bleed was spontaneous or precipitated by injury
Is rodenticide used on the property?
Pro tip: Don’t ask if there is access to rat bait as a lot of owners don’t believe their dog can get to it and will say no.
Does your pet live in an enclosed yard or apartment building?
Snakes can cause coagulopathies, and are a common in some areas. However, it if the pet lives in an enclosed yard or inside an apartment building then snake bites are less likely, unless they are walked or have a property near bushland
History of previous successful surgeries?
Yes? Unlikely congenital
Current medications?
Some medications can cause a thrombocytopaenia although rare to be severe enough to cause spontaneous bleeding.
3. Consider the signalment
Amazingly the signalment can give us a good idea as well.
Young dog: Due to their inquisitive nature, snake bites or rodenticide are more likely.
Very young: Congenital should be considered, although they can be just as inquisitive.
Older patients: Tend to behave themselves and therefore are more likely to get acquired diseases.
Doberman: Prone to primary platelet factor disease, Von Willebrands.
Devon Rex: Prone to secondary coagulation disease
Greyhounds: Excessive breakdown of formed clots, fibrinolysis syndrome.
You may already have a likely diagnosis in your mind, or have a narrowed differential list just from these history questions and considering the signalment.
In my roles as hospital director and performance coach, I frequently hear: “I want to have work-life balance”.
This is a statement I have seen time and time again ruin people’s perception of their careers, and their sense of happiness. Why? Because not one person has been able to answer the question I follow up with – and that is: “What does work-life balance look, feel and sound like for you?”
I get a stunned silence – which, to me, highlights the fact they are chasing something they have no clarity about.
Here are some things to consider:
Work-life balance is individual
If you are happy doing something and love it, but someone else tells you that you don’t have work-life balance… ignore them.
What work-life balance means for him or her has nothing to do with what it means for you.
Discover what it means to you
Think about the main areas in your life that are important to you. The most common things said by people I coach are family, friends, adventure and health.
Now, think about how often and how much time you need to spend in those areas to be fulfilled, but not overindulged. If, for you, it is catching up with your friends once a fortnight and exercising four times a week, then schedule it in.
Make it happen.
Be realistic
If you have just finished university and started your career, an internship or residency, then you have to work hard to apply what you have learned, and learn more – that’s just how it is for the first couple of years.
If you want to achieve more for yourself, then just accept that classic work-life balance may not be realistic for a period of time, but also know you are preparing your future self for success.
Next time you hear someone mention work-life balance, remember it is personal – you have to define it, communicate it, then schedule it, and be realistic for the stage in your career and the pathway you have chosen.
True work-life balance takes action, consistency and commitment.
You’re stuck in the clinic in the middle of the night with a dog that is dying – it’s bleeding into its abdomen and needs blood, but the bag in the fridge is expired.
You’ve heard it’s possible to collect the blood out of the abdomen and safely give it to the patient, but you’re not sure how and don’t have time to google. How do you actually do it?
It’s easier than you think. Depending on what equipment you have available in the clinic, here are two practical ways of administering an autotransfusion.
Collection
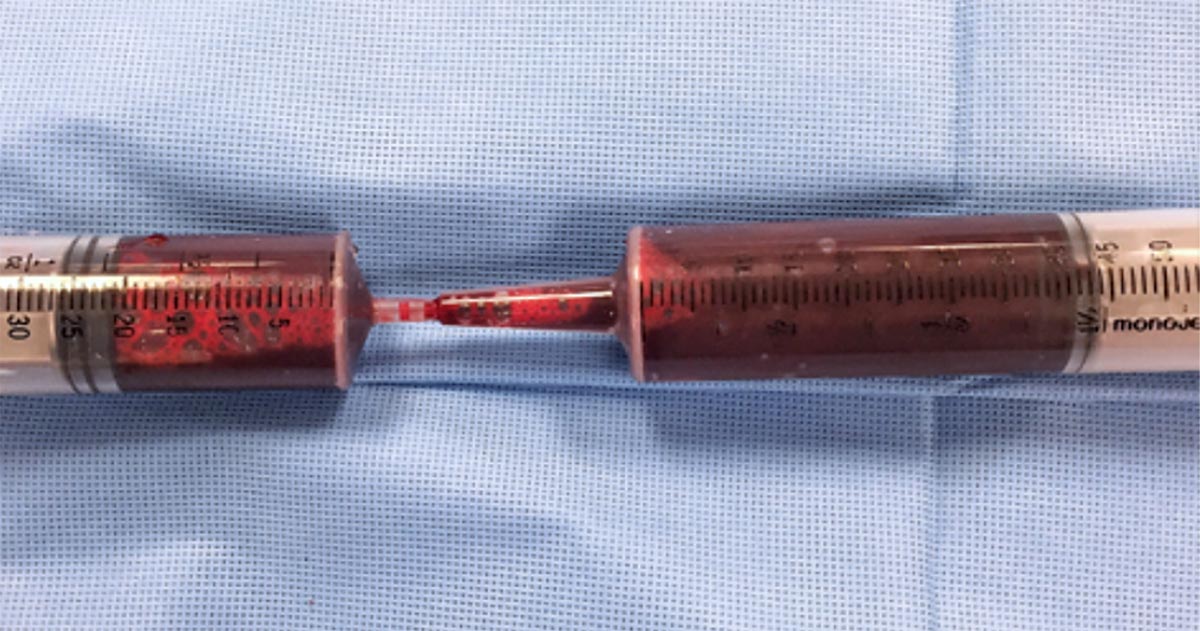
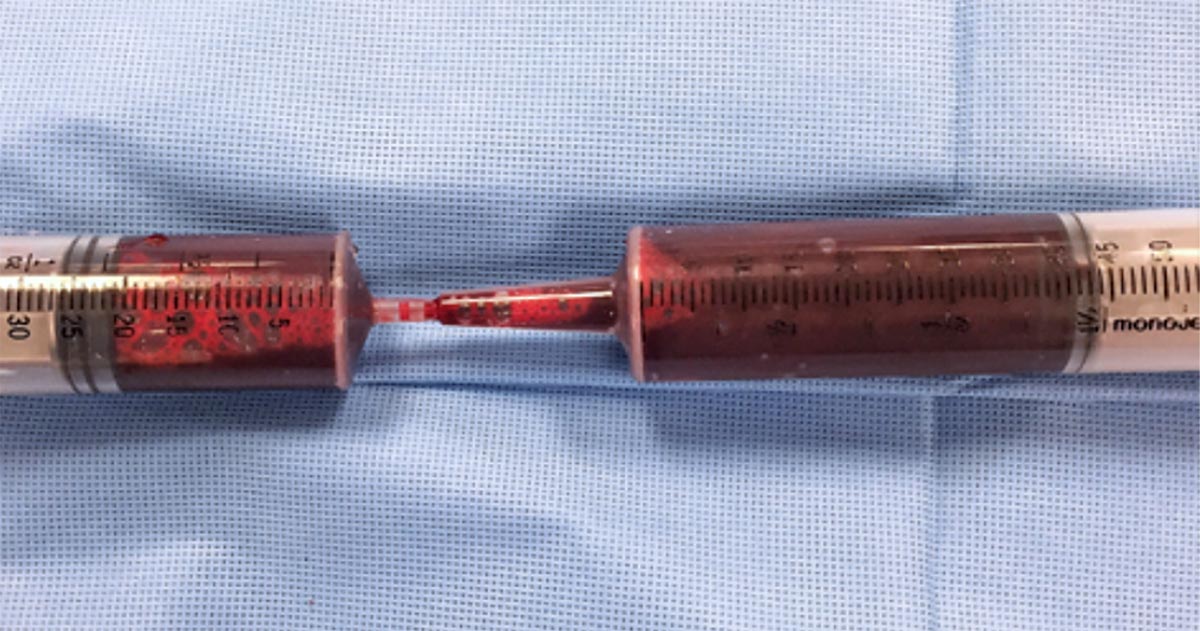
Blood can be collected from the abdomen or thorax during exploratory surgery, simply by sucking it up with a 60ml syringe.
Time is usually of the essence in these cases, so a handy tip is to use 60ml catheter tip syringes to aspirate the blood, then get someone to transfer the blood into a standard Luer-tipped syringe by shoving the smaller tip into the catheter tip. Like this:
Besides the faster collection time, the bigger aperture of the catheter tip syringe will also reduce negative pressure during collection and, therefore, the chances of haemolysis.
If you are not going into surgery, you can collect the blood percutaneously – using a butterfly needle or catheter – as you would drain any body cavity fluid.
You shouldn’t need to add any anticoagulants to your syringes, as fibrinolysis has already occurred – meaning the blood shouldn’t clot in your syringe.
Administration
Whichever method you use, it’s crucial the blood is administered through a blood filter.
Method one
The most straightforward way is to simply inject the blood back into the patient using the Luer-tipped syringe through a filter. For this technique, you will need a filter that can connect to a syringe.
Method two
If you only have a blood filter as part of a blood giving set, you could use a two-way stopcock valve to get your collected blood into a sterile bag – like an empty IV fluids bag, or a dedicated blood collection bag – and then run the blood through your blood giving set with the built-in filter, as you would for a normal transfusion.
This is a bit more fiddly, so adding a few little blood filters to your emergency equipment could be well worth your time.
When you shouldn’t do it
Autotransfusions are most useful in cases of bleeding due to clotting deficiencies where the clotting problem is already being addressed, but a need for red blood cells still exists; and for cases of traumatic or postoperative bleeding.
It is contraindicated if contamination with urine, faeces, bile or bacteria – in case of septic peritonitis – is likely; or in cases of neoplasia in the body cavity where an autotransfusion has the potential to seed neoplastic cells to the rest of the body.
A while ago, I did a Q&A session at the RVC in London and one of the most popular questions was: “How do you reset in between emergencies and consults?”
As an emergency vet this is critical, but when I think about it, this is critical for the success as a vet in general. In emergencies, we might triage several crashing patients at the same time, but in general practice this is similar to a fully-booked Saturday morning consult shift, together with unexpected walk-ins.
Control-alt-delete
Over time we develop some way of resetting so we are able to do what we need to do and, more importantly, not carry baggage from the day and each consult into the next ones. This could be some kind of routine, ritual or process. It takes time and practice, but it is essential for mental well-being and being present with each patient and owner.
What would happen if we improved our ability to reset? For me, I saw a noticeable improvement in my performance on shift; I was able to clear my thoughts faster and focus on what was in front of me.
I think of it being similar to going to the gym – you start doing weights and, with time, you get stronger. But, if you get in the right head-space, focus on your form and movement, you get better results faster and with less injury.
Think about it
The more conscious you are of anything you do, the better you perform at it. So, if you were more conscious and deliberate with your resetting process, imagine how that would impact your performance – and imagine the impact on your consults or on your team.
I started thinking about my resetting ritual several months ago. First, I noted it down then started to experiment and try different things. This made me create a ritual that was better, faster and was more effective.
My reset ritual before each consult goes like this:
I adjust my shirt and my name badge to make sure I look professional – if I was a client, I would like my vet to look neat and presentable, and not covered in fluff or worse.
I adjust my stethoscope – it’s like a magical amulet, and I have associated many positive memories with it. When I wear it I feel I’m the best version of myself. It reminds me of the education I have had, what I know and the experience I have.
I feel for my pen while I read over the clients name, the pets name, age and sex – I am ready to introduce myself, to greet the pet and to take notes.
Deep breath in, then out – this brings me back to the present. I clear any thoughts of what I have to do, what happened to the last pet and how much work is piling up.
Open the door, smile, introduce myself and BE PRESENT.
Renewed focus
I do this every time I open the consult room door, it only takes 10 seconds to reset as I have practised this hundreds of times and I know the purpose of each step. Even if my mind is not quite ready, the movements and physical actions help to focus my mind.
My transition ritual has helped me greatly in connecting with clients and gaining their trust, which, in return, helps their pets and makes my experience of my career more enjoyable.
Few companies now offer affordable point-of-care tests for canine C-reactive protein (CRP). As we did when we recently received our new box of CRP slides, you might soon be asking the question: what do we even do with this stuff?
Here’s what we’ve learnt…
CRP is one of the acute phase proteins produced by the liver in response to inflammation. Healthy patients have very low levels of CRP, but a systemic inflammatory condition will cause an increase in CRP within four to six hours. Conversely, increased levels will decrease rapidly on resolution of inflammation. This provides an almost real time measure of inflammation that is more responsive and reliable than the white blood cell response.
In other words, CRP can indicate the presence of inflammation before the patient’s white blood cell count gives any clues, or before it becomes pyrexic – and, unlike the white blood cell count, stress and steroids do not affect CRP levels.
Uses
So, how do we use it?
I love it for early pickups of problems in those grey area cases: the dog seems okay on clinical examination, but something about it bothers me. A normal or mildly increased CRP test will make me sleep more easy, while a surprise high reading will prompt me to admit for full diagnostics, or at least get the patient in for a follow-up CRP the next day. Conversely, a localised problem – such as an abscess – combined with a normal CRP test might mean you can hold off on antibiotics and just recheck CRP in 24 hours.
It’s great for monitoring response to treatment. If my plan is working then I’d expect CRP to show a significant decrease by day two or three. If it’s not dipping by then, I need to reassess my treatment plan. Do I need to change antibiotics? Scan it again? Maybe we need to consider surgery? It can also be a good prognosticator. Research has shown failure of CRP to decrease significantly (around a 3× decrease) by around day three is generally bad news for patients with inflammatory conditions such as pancreatitis and immune-mediated haemolytic anaemia.
We are starting to play with it for post-surgical monitoring. Any surgery will cause inflammation with an increase in CRP levels, but in an uncomplicated postoperative period, you should expect levels to start decreasing by day three to five. A base line CRP 24 hours after surgery with a recheck on day three should pick up early signs of postoperative problems such as infection, and prompt investigation or intervention.
A potentially nifty use for it that we haven’t yet had the opportunity to use is in differentiating inflammatory lamenesses (arthritis, infection, injury) from a neurological causes – that is, is it arthritis or a nerve problem?
Limitations
Remember, it’s very sensitive, so will increase with almost any inflammation. A mild upper respiratory infection or a bad gingivitis will likely induce some changes, so it’s important not to over-interpret (keep in mind that the magnitude of the increase in CRP does generally correspond with the severity of the inflammatory response). A pancreatitis case where the CRP fails to drop does not always mean death is looming – you may have just missed the concurrent skin disease. Always interpret CRP values in concert with your clinical examination.
Be aware that pregnancy and intense exercise can increase CRP values.
Not all serious conditions have an inflammatory component. CRP will be unchanged in most veterinary cases of heart disease; in common hormonal disease, such as adrenal disease and uncomplicated diabetes; urinary obstructions; many localised cancers; epilepsy and many others. Don’t presume that just because CRP is normal, everything is fine.
No similar test exists for cats.
Sit up and say…
My favourite way to explain how to use this test is by using its highly appropriate acronym – any unexpected increase should make you sit up and say: “Oh CR*P! What am I missing?”
Last week we discussed the causes and diagnostic pathway for investigating immune-mediated thrombocytopenia. This week we will go through the management of this condition.
Despite the fact red blood cells are not actually being destroyed, a severe anaemia can develop from blood loss due to coagulopathy – a common reason for why they present to emergency practices. The management of these patients is broken down into three main areas:
improving oxygen delivery
commencing immunosuppression
management of the underlying cause (if identified)
Optimising oxygen delivery in the acute phase is going to keep them alive long enough for immunosuppression to work. This is achieved through IV fluids to help improve perfusion and blood transfusions to replace red blood cells. If fresh whole blood is available, it can assist in increasing platelet numbers, but generally it is not very effective.
Platelet transfusions using platelet-rich plasma can be considered if it is available. Plasma transfusion is not effective at managing the coagulopathy as it is due to a loss of platelets, not a loss of coagulation factors.
Immunosuppression
Large areas of ecchymotic haemorrhage on the skin are a quite obvious sign of thrombocytopenia.
Immunosuppression therapy is often commenced concurrently as the patient is being stabilised.
The first choice is either dexamethasone 0.5mg/kg IV every 24 hours if the patient is not stable enough for oral medications; otherwise, once stable, start prednisolone at 2mg/kg by mouth per day divided every 12 hours.
Other immunosuppressive agents include:
Azathioprine – 2mg/kg by mouth every 24 hours then 0.5mg/kg by mouth every other day. The main concerns are bone marrow suppression and hepatoxicity – also, it is very toxic in cats.
Ciclosporin – 5mg/kg to 10mg/kg by mouth divided twice a day; cats 5mg/kg by mouth every 24 hours.
Chlorambucil could also be used at a dose of 0.1mg/kg/day to 0.2mg/kg/day by mouth if the response to prednisolone is insufficient.
Management
Management of the underlying cause should be commenced if a cause is identified, but this is often not the case.
Other management options include:
Vincristine can be trialled to increase platelet number as it stimulates the release of platelets from the bone marrow.
Gastroprotectants can be considered if gastrointestinal bleeding has occurred – these include proton pump inhibitors and sucralfate.
Strict confinement, potentially sedatives and minimal blood sampling are important to minimise injury that may result in further bleeding and blood loss.
Antithrombotic therapy is not part of standard management as, unlike immune-mediated haemolytic anaemias, thrombotic events rarely occur.
When it comes to monitoring, platelet counts are performed daily until more than 40 × 109/L – this can take up to two weeks to occur.
Once above this level, take weekly counts until the numbers have normalised. Once they have, taper immunosuppressive medications over four to six months, with 20% dose reduction every couple weeks, generally with the adjunctive immunosuppressants first and prednisolone last.
Our scavenger hunt enjoyed 138 entries, of which the winners and their corresponding prizes are detailed below. Congratulations to all winners – particularly our overall winner Gem Harrison, who will be the recipient of a coffee machine.
Our other winners are:
VTX COURSE: Elizabeth Woodall
VTX MEMBERSHIP: Katrina Bailey
VET CT HAMPER: Rebecca Curtis
SPILLERS GOODIES: Diane Fancourt
BVNA TICKET: Adele Jones
EMPOWERING SOCIAL MEDIA CLASSES: Emily Harvey, Rebecca Wakeham and Gillian White
Thrombocytopenia is a condition characterised by a decrease in platelet numbers, which is often caused by increased destruction of platelets or a decrease in production.
Thrombocytopenia can manifest in many ways – the signs can be subtle and easily missed, such as small petechiae on gums, or quite obvious signs, such as large areas of ecchymotic haemorrhage on the skin.
Ecchymotic haemorrhages are often attributed to disorders of secondary haemostasis, such as rodenticide intoxication, but it can also occur with thrombocytopenia depending on the severity and chronicity.
Other common clinical signs include:
epistaxis
blood in stools, urine or vomit
pale mucus membranes
lethargy
weakness
Therefore, the first step to managing a patient with a severe thrombocytopenic episode that has resulted in significant blood loss is to manage shock, if present, with IV fluids, then administer a red blood cell transfusion.
Patient handling
Careful patient handling is critical as these patients can bleed easily, leading to blown veins, large bruises that contribute to the development of anaemia and significant patient discomfort. Beyond initial patient stabilisation, the next step is to determine the underlying cause.
Diagnosing thrombocytopenia is relatively straightforward with the demonstration of low platelet counts. Generally, bleeding does not occur until the platelet count drop below 40,000 thousands per cubic milliliter (k/uL). This can be determined by either a haematology machine or manually via blood smear analysis.
When assessing blood smears, the general rule is one platelet per high-powered field on the monolayer is equal to 15,000k/uL. With either method, you must assess for platelet clumping on a blood smear as this can artefactually drop platelet numbers, leading to a false diagnosis.
The diagnostic pathway should not stop there. It needs to continue to determine the underlying cause.
The most common cause of thrombocytopenia is immune-mediated destruction. This can be either a primary (diagnosis of exclusion) or secondary cause (such as Rickettsia infection, and drugs such as sulphonamides, toxins and neoplasia). Other less common causes include:
splenomegaly, which can lead to platelet sequestration
disseminated intravascular coagulation and acute blood loss, leading to platelet consumption
bone marrow disease, which results in reduced platelet production
Signalment and history will refine such a diagnosis, as certain breeds are more prone to developing thrombocytopenia than others – for example, grey collies due to a defect in haematopoietic stem cells, and whippets and greyhounds, which traditionally have a lower platelet count than other breeds.
The generally diagnostic pathway continues to include haematology and biochemistry, thoracic radiographs, abdominal ultrasound and depending regional prevalence testing for infectious organisms with PCR and ELISA assays.
Next week I will cover the management principles of the thrombocytopenic patient.
Several easy and affordable ways exist to measure lactate in general practice, which means the clinical applications of monitoring lactate is no longer the reserve of specialist and emergency centres.
But why and how should you be using it in general practice?
What is lactate again?
When oxygen is not effectively delivered to cells throughout the body – which, in our patients, will mostly be due to hypoperfusion (for example, hypovolaemia, vasodilatory shock and cardiac disease) – cells will switch from aerobic to anaerobic metabolism to stay alive.
Think of anaerobic metabolism as the fuel-powered generator that kicks in during a power cut – it’s not as good, but it’ll keep the lights on for a while. However, unless the power comes back on, the generator will eventually also fail and plunge you into darkness.
Lactate is the end product of this process of anaerobic metabolism. To be clear, lactate is not the bad guy – in fact, it plays an important role in keeping the cells going until they have access to sufficient oxygen again. It’s simply the bearer of bad news.
Because lactate is the harbinger of doom; it’s the leading horseman of the apocalypse…
When lactate is high, you should stop whatever else you are doing and pay attention to the patient in question – this patient is probably surviving on anaerobic metabolism. It is critically ill and possibly heading for a long walk in the great park in the sky…
How should I use it?
It is valuable in any patient with any serious illness or injury. Things that should make you consider checking lactate would be:
slow capillary refill time
any mucous membrane colour other than a nice, healthy pink
increased heart rate
weak or bounding pulses
significant dehydration
depressed mentation
history of major trauma
major infections
significant blood loss
any disease that has the potential to progress into a life-threatening condition
…basically, any animal sick enough to make you worry about it possibly dying.
Run it with your initial diagnostics to get a baseline level, and run it within 10 minutes of taking the sample.
What do I do about my results?
Normal range
What do my results mean?
< 2.5 ?
3-4 ? ?
4-6 ? ?
> 6 ? ?
(levels in mmol/L)
If it’s within the normal range then check regularly – ideally until your patient is well on its way to a full recovery.
Lactate levels may start increasing in response to hypoperfusion before the patient starts showing overt signs of deterioration – the fuel in the generator hasn’t run out yet – which makes it a very useful monitoring tool to detect problems early on.
We find a six to eight-hourly check in very sick patients will pick up deterioration fast enough to give you time to react, while a twice-a-day check in more stable animals will suffice.
Elevated
If it is increased at any point, you need to focus immediately on trying to reduce it.
This usually means starting with fluid boluses for shock. Recheck lactate one hour after initiating the appropriate therapy. Your goal is for the lactate value to be reduced by approximately 50% within one to three hours (ideally one hour) of initiating therapy. If it’s coming down nicely then keep checking every two to three hours.
You want it to be back to normal within 24 hours (48 hours max).
Nothing working?
If it has not decreased as expected – or, especially, if it increases despite treatment – it means things are going seriously wrong. At this stage you need to:
Devote all your attention on trying to find and correct the underlying cause while you adjust your emergency therapy to address hypoperfusion.
Speak to the owners.
If you do not have the time, facilities or experience to deal with shock cases, you need to consider referring the patient to a specialist centre urgently for stabilisation, if this is an option available to you.
Remember…
Intense exercise, muscle tremors and seizures are associated with anaerobic muscle activity and can, therefore, cause significant increases in lactate levels (the cause of the “deep burn” when you’re dying in that CrossFit class). This can also occur when a patient resists when you are taking blood, or starts trembling in fear the moment it walks into the clinic, which can cause misleading lactate results.
Puppies can have a higher “normal” level of plasma lactate up to seven months of age.
Anaemia does not generally cause hyperlactataemia unless it is very severe, but by this stage you shouldn’t need lactate to tell you the patient is in serious trouble.
Having said that, normal lactate levels that suddenly start climbing in a hospitalised “stable” anaemic patient could be the push you need towards giving that blood transfusion.
Ionised hypocalcaemia (iHCa) is a well-known electrolyte abnormality in critical human patients, which is also beginning to be recognised in our critical feline and canine patients.
The exact mechanism for the development of iHCa is still unknown – making prevention difficult, if at all possible. Controversy also exists as to whether treating iHCa is of any benefit, especially in non-clinical cases.
Despite these issues, serum concentration is proving to be an accurate prognostic indicator for the morbidity and mortality rates of some of the more critical patients.
Research
Over the past 30 years, significant resources have been put into trying to demystify the pathophysiological causes of iHCa in critically ill people; however, the exact mechanisms are still to be determined.
Some proposed mechanisms include:
abnormal parathyroid hormone secretion or function
abnormal vitamin D synthesis or function
hypomagnesaemia
calcium chelation
alkalaemia
calcium sequestration in tissue or cells
an increase in calcitonin precursors (procalcitonin)
In a canine study where endotoxaemia was induced, it was found hypovitaminosis D was associated with iHCa (Holowaychuk et al, 2012).
Veterinary studies
The true incidence of iHCa in critically ill canine and feline patients is yet to come to a consensus, due to the limited veterinary studies.
In one retrospective study, 90% of 55 cats with septic peritonitis was reported to have iHCa (Kellett-Gregory et al, 2010), while only 24% of septic dogs (n=58) was reported to have iHCa (Luschini et al, 2010).
Regardless of the true incidence, the commonness of this change questions whether a need exists to treat iHCa, especially cases in the mild or non-clinical categories.
No consensus
At this stage, no consensus exists to either support or prohibit the treatment of hypocalcaemia in critically ill patients.
Well-designed prospective studies are scarce in human literature and non-existent in the veterinary field; no evidence-based guidelines are available for treatment.
Based on logic, arguments for the administration of calcium to critically ill patients include:
iHCa during hospitalisation is a negative predictor for morbidity and mortality of patients.
Hypocalcaemia can cause decreased myocardial contractility.
In hypotensive patients dependent on vasopressors or inotropic agents, the supplementation of calcium may be beneficial.
Arguments against calcium supplementation include:
Calcium accumulation within cells predisposes to hypoxia and ischaemia-reperfusion injury.
Increased mortality in experimental models of sepsis when calcium is supplemented, on top of the lack of evidence to support this act.
Prognostic use
Serum calcium concentrations – or, rather, the trend of it in hospital – appears to be of valuable prognostic indicators.
Kellett-Gregory et al (2010) found although no direct associations existed between the presence or severity of iHCa at the time of patient admission, a positive correlation existed between the lowest iCa post-hospitalisation, and the length of hospitalisation and duration of intensive care stay.
Of the cats that had iHCa, those that failed to return to a normal ionised calcium (iCa) during hospitalisation had a significantly lower rate of survival to discharge. Interestingly, iHCa was not associated with the status of hypotension, coagulopathy or arrhythmias, so cannot be used to predict the occurrence of these.
These findings were echoed by Luschini et al (2010), where low mean ionised calcium and lowest documented ionised calcium concentrations were found to be associated with a poor outcome. The severity and duration of iHCa appears to be important in determining prognosis in these patients.
Conclusion
Controversy exists regarding whether treatment of mild iHCa in critically ill patients is recommended; however, one thing we now know is serum iCa concentration is a reliable predictor of mortality and morbidity in canine and feline patients.