Establishing client rapport is paramount to any consultation. Without client rapport, trust is difficult to establish and clients are less likely to follow your recommendations.
Tip #1: Never forget to greet the pet.
We have seen a good deal of negative publicity regarding veterinary surgeons in the media, so now, more than ever, we need to build that trust from the moment the client and their pet walk into the room.
Here are 5 tips to help you build rapport:
Never forget to greet the pet. This should come naturally to most of us, but if it doesn’t, do it often so it becomes a habit.
Ask open-ended questions that enable you to get to know your client and their pet. This will help you understand more about how their pet fits into the client’s lives and helps you understand their situation. Use more focused, close-ended questions for getting specific details later.
Listen! Listening skills are very important. Try not to cut the client off and listen to their concerns. There is sometimes a disconnection between what you think your client’s concerns are and what they really are. If you are uncertain what their main concerns are, then ask.
Empathy. We can sometimes forget what it feels like to be on the other side of the examination table. Place yourself in your client’s shoes and remember they love their pet enough to have brought it in to see you, and are counting on you to help get their pet better.
Be honest, sometimes you don’t know what is going on. By establishing rapport, you can work together with the client to develop a plan that is best for their pet.
According to PDSA [PDSA Animal Wellbeing (PAW) Report 2022], rabbits are the third most popular pet in the UK behind dogs and cats. With an estimated 1.1 million pet rabbits in the country, that’s about about a tenth of the population of pet dogs and cats, which hover around the 9 to 10 million mark.
So, if the pet ratio of dogs/cats:rabbits is 10:1, why isn’t this reflected in our teaching? Despite rabbit populations being endemic to the UK for more than a thousand years, they always seem to get lumped with guinea pigs and the cold-blooded pets like lizards and corn snakes when it comes to textbooks or university curriculums.
I can confidently say my education on rabbit physiology and medicine has been dramatically less than 10% of what I’ve received for small animal medicine. Perhaps this is why many vets, especially new or recent graduates, feel more confident handing off any rabbit patients to the resident “expert” of the practice or even referring to an exotics specialist, rather than seeing it themselves.
Accessibility
It’s a sad truth that the less convenient education and health care are to access, the less people will reach for them. By extension, the less veterinary practices that advertise care for rabbits (and other exotics), the less rabbits are likely to be registered at a practice and receive regular preventive care.
For example, as a native to the land of Kent, I only know of two or three practices that would call themselves “exotic specialists” and I know that, for a lot of rabbit owners, traveling half way across the county to visit one of these few practices would not be practical or plausible. Perhaps this is why, according to PDSA reports, at least 11% of pet rabbits receive no preventive health care, including vaccinations.
Rabbits are a social species that has evolved to live in groups, not alone.
Education
The value of a veterinary consultation is not simply to talk through clinical signs or address a flea outbreak in the home, it’s a chance for owners to discuss management issues or to ask for general advice. When rabbits aren’t brought in for routine consultations, then discussions about their diet, husbandry and behavioural needs don’t get to be had.
Some vets are already worried that the development of an annual rabbit haemorrhagic disease (RHD) booster rather than biannual is going to dramatically reduce rabbit welfare by halving the number of times these pets receive a clinical exam.
Welfare
Of course, like all “exotics”, there’s the argument to be made as to whether these animals are suitable pets in the first place. Personally, I feel that this is a moot point for the time being.
The fact that more than 50% of pet rabbits are housed by themselves with no companionship speaks volumes about the lack of knowledge the general public possesses on how to care for these animals. However, with more than a million of them currently out there, they’re not going away anytime soon.
The best we can do as professionals is educate our clients so welfare can be maximised as much as possible… and that starts with educating ourselves. I hope that in the near future the landscape of the veterinary degree can shift to better reflect the current demand for exotic vets – or at least rabbit vets.
This patient was brought to us for exercise intolerance, breathing difficulty and loud airway sounds.
The patient has laryngeal paralysis. This is where the muscles controlling the arytenoids cartilages do not work and leads to failure of opening of the arytenoids during inspiration.
Most commonly seen in middle-aged large breed dogs, it can occur acutely, but more often it is a chronic problem exacerbated by heat or stress. The cause is often unknown, but it can be caused by trauma or lesion to the cervical region or some kind of neuropathy, such as myasthenia gravis or tick paralysis. Diagnosis is based on visualisation of the arytenoid cartilages failing to abduct during inspiration under light anaesthesia.
Treatment
The management of the acute presentations include oxygen and sedation (butorphanol) to improve airway dynamics – with or without active cooling triggered by heat and with or without anti-inflammatories (dexamethasone) to reduce swelling secondary to airway turbulence.
Patients in severe respiratory distress, anaesthesia and intubation may be required for a short period. Long-term management involves either surgery, such as laryngeal tieback, or conservative management strategies that involve weight loss, avoiding exercise and being kept in a cool environment.
Idiopathic acute haemorrhagic diarrhoea syndrome (AHDS) – previously known as haemorrhagic gastroenteritis – remains the one disease where constant debate exists as to whether antibiotics should be used as part of the standard treatment.
The logic behind using antibiotics to prevent bacterial translocation is sound, and if AHDS is truly initiated by Clostridium species or their toxins then the use of antibiotics can be justified.
However, no knowledge exists of the true frequency of bacterial translocation in AHDS patients and conflicting evidence supports Clostridium being the initiating cause of AHDS in dogs.
Together with new data indicating the use of antibiotic therapy in aseptic AHDS patients did not change the case outcome or time to recovery, the benefit of using antibiotics must be weighed against the very real risk of selection of antibiotic resistance and other complications associated with inappropriate antibiotic use.
In this blog, we will explore the evidence against the use of antibiotics in AHDS.
Cause unknown
AHDS is characterised by an acute onset of vomiting (of less than three days’ duration) that can quickly progress to haemetamesis, and severe and malodorous haemorrhagic diarrhoea, accompanied by marked haemoconcentration that can be fatal if left untreated.
AHDS is a diagnosis of exclusion; other diseases (such as canine parvoviral enteritis, thrombocytopenia, hypoadrenocorticism, azotaemia, hepatopathy, neoplasia, intussusception, intestinal foreign body and intestinal parasitism) must be ruled out by a combination of medical history, vaccination status, complete blood count, serum biochemistry, coagulation times, diagnostic imaging and faecal testing.
Small breed dogs – in particular, the Yorkshire terrier, miniature pinscher, miniature schnauzer and Maltese – have been found to be particularly predisposed. On average, the affected dogs were young (a median of five years old).
The cause of AHDS is still unknown. Clostridium perfringens and its toxin has been incriminated as being the initiating cause; however, conflicting studies have refuted this claim. It is also difficult to determine whether overgrowth of Clostridium speciesis primary or secondary to the intestinal injury.
Virus theory
Another theory is viruses may have a role in AHDS’ aetiology. At this stage, only single agents had been investigated. It is possible a novel agent not yet been tested is the cause of this syndrome, or possibly the syndrome is the result of a very complex interaction between multiple organisms or their toxins.
For the aforementioned reason, no indication exists for the use of antibiotics to treat for the underlying cause.
Another argument behind the use of antibiotics lies in the fact most idiopathic AHDS patients have several risk factors for bacteraemia.
Necrosis of intestinal mucosa, leading to the disruption of the gastrointestinal mucosa-blood barrier; adherence of significant numbers of bacteria to the necrotic mucosal surfaces that increases the risk of bacterial translocation; significant hypoalbuminaemia indicating substantial loss of mucosal epithelial layer; splanchnic and intestinal hypoperfusion, leading to reduced intestinal barrier function; and microbial dysbiosis all contribute to an increased risk of bacterial translocation.
Although bacterial translocation has the potential to lead to sepsis, the true incidence of bacterial translocation needs to be established in idiopathic AHDS patients, as well as their influence on the outcome of the patients.
Antibiotic requirement
Use of unnecessary antibiotics not only disrupts the protective mechanisms of a normal intestinal microflora, but also the real risk of post-antibiotic salmonellosis and Clostridium difficile-associated diarrhoea.
Multiple studies have suggested antibiotics are not required in the treatment of aseptic idiopathic AHDS patients.
In a prospective study of bacteraemia in AHDS dogs by Unterer et al (2015), the incidence of bacteraemia of patients with idiopathic AHDS was 11%, compared to those of healthy controls, where it was 14%.
Transient bacterial translocation to mesenteric lymph nodes occurred in 52% of dogs undergoing elective ovariohysterectomy (Dahlinger et al, 1997), and confirmed in studies by others (Harari et al, 1993; Howe et al, 1999; Winkler et al, 2003), where portal and systemic bacteraemia was reported in clinically normal dogs.
As long as the immune system is competent, and the functional capacity of the hepatic reticuloendothelial system is not overwhelmed, the body is usually effective at eliminating organisms from the blood.
This is reflected in the Unterer et al (2015) study result, where – regardless of the bacteraemia status – all idiopathic AHDS dogs survived to discharge.
In another prospective, placebo-controlled, blind study by Unterer et al (2011), idiopathic AHDS patients were either treated with amoxicillin/clavulanic acid for six days or a placebo, and no significant difference occurred between the treatment groups concerning mortality rate, duration of hospitalisation or severity of clinical signs.
They concluded, without the evidence of sepsis, antibiotics do not appear to change the case outcome or shorten the time to recovery.
Negative impacts
The negative impacts of inappropriate antibiotic use are undeniable – especially in a time where resistance has become a worldwide public health concern.
Use of unnecessary antibiotics not only disrupts the protective mechanisms of a normal intestinal microflora, but also the real risk of post-antibiotic salmonellosis and Clostridium difficile-associated diarrhoea.
With evidence all pointing against the use of antibiotics as routine treatment of aseptic idiopathic AHDS, next time you are about to reach for antibiotics, I urge you to reconsider. Although it has taken some time to adopt and requires clear communication with clients, all vets should feel comfortable not using antibiotics for AHDS patients.
I cannot stress enough how crucial it is to develop a systematic approach to doing ultrasounds. Not only will this approach help develop an anatomic mind map, it will also safeguard you from accidentally overlooking organs.
When examining each individual organ, the same theory applies. This will ensure you look at each organ in its completeness, reducing the chance of an abnormality being missed.
The only way to improve your ability to track through organs is by repetition; repeating and practising the same manoeuvres over and over again. In time, you will notice you will be able to detect subtle changes you wouldn’t have been able to before.
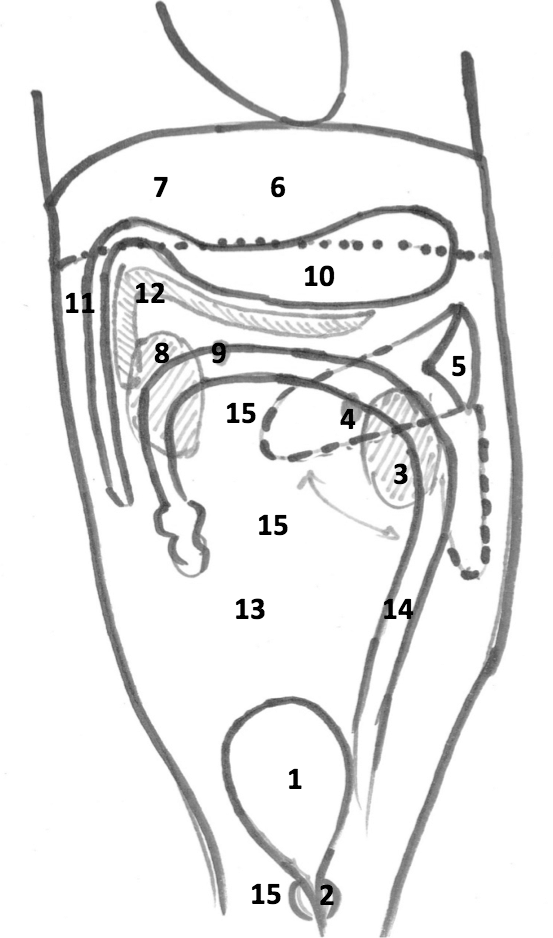
Suggested scanning procedure
Starting at the bladder and moving anti-clockwise:
Abdominal ultrasound is an invaluable diagnostic tool that can give us far more information about abdominal organs than radiographs. It can also be a very daunting procedure – especially for clinicians unfamiliar with how the machine operates.
One of the biggest frustrations with using the ultrasound machine stems from not knowing what each button is for, or how to use them to adjust the image quality appropriately, to obtain the information required.
Over the next few posts, I will offer you hints and tips on how to get started. Once you understand what all those buttons and dials are for, you should be able to operate just about any ultrasound machine with confidence.
I will also explain how to perform an abdominal ultrasound in a systematic manner, as well as how to get the most information out of it.
Buttons and their uses
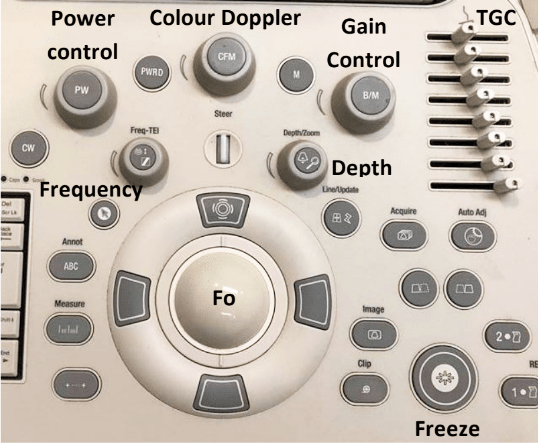
Figure 1. An ultrasound machine control panel.
Figure 1 is an example of a typical ultrasound machine control panel. The following explains the different buttons and dials present, and their uses.
Power control
The power or output control affects the strength of the emitted sound pulse. Keep this to as low as possible for the required depth.
Gain control
The gain control regulates amplification of all returning echoes non-selectively – that is, it makes the entire image brighter.
Time gain compensation
The time gain compensation (TGC) selectively regulates amplification of echoes returning from various depths.
The objective of TGC is to provide a uniform image from top to bottom. Returning near-field echoes are already strong and may actually need to be suppressed. Far-field echoes are weaker and, therefore, may need to be amplified more according to the depth from which they return.
Depth
The depth allows you to choose how deeply into the tissues the image will display. Use an appropriate depth to view the structure of interest – that is, adjust the depth so the structure fills three-quarters of the field of view.
Focus
The focus (Fo) provides the best image at a certain depth and should be adjusted so it is at – or just behind – the area of interest. The focal point is the yellow arrow on the right side of the screen, which can be moved up and down with the Fo tracking ball.
Freeze
The freeze-frame control creates a frozen on-screen image for closer inspection, annotation, measurements using electronic calipers and producing permanent documentation with digital, film or paper images.
Clip
The clip button records a short video clip.
Colour Doppler
The colour Doppler assesses fluid flow. It is useful for differentiating between a vessel and structure of equal echogenicity, such as an adrenal gland or lymph node, and for determining the vascularity of a structure, such as a torsed spleen, mass lesion or abscess.
Flow towards the transducer = red, while flow away from the transducer = blue.
In patients with respiratory compromise, it is important to look at the respiratory components of the blood gas to determine both oxygenation ability and adequacy of ventilation.
To assess oxygenation, the partial pressure of arterial oxygen (PaO2) to fraction of inspired oxygen (FiO2) ratio, and alveolar-arterial gradient (A-a gradient) can be used. Conversely, the partial pressure of carbon dioxide (PCO2) is what dictates the adequacy of ventilation.
Before going further, it should be noted only arterial samples can be used to evaluate oxygenation. Peripheral venous blood samples are rarely useful for oxygenation assessments, as the values are highly influenced by local factors and the degree of occlusion of the vessel from which the sample was collected from.
Ventilation, conversely, can be assessed from either venous or arterial samples. The PCO2 values from the arterial samples are usually about 5mmHg to 10mmHg lower than the corresponding venous sample.
Abnormalities
Oxygenation and ventilation are not interchangeable terms. Adequate ventilation does not necessarily equate to adequate oxygenation, and vice versa.
Oxygenation is determined by efficiency of oxygen absorption into the blood stream, after passing through the lungs, then delivered to the tissue. It is dependent on both ventilation (V) and perfusion (Q).
For proper oxygenation to occur, matching ventilation and perfusion must occur at the level of the alveoli. When a V/Q mismatch occurs, blood is not properly oxygenated after passing through the lungs, referred to as venous admixture.
Three forms of V/Q abnormalities exist:
Low V/Q can be caused by:
pneumonia
asthma
pulmonary oedema
inflammation
pulmonary thromboembolism
pulmonary neoplasia
Absent V/Q means blood has been diverted from parts of the lungs that are inadequately ventilated, such as those caused by atelectasis and alveolar collapse secondary to severe pleural effusion.
Diffusion impairment is caused by an increased distance between the gas exchange surfaces and pulmonary arterioles (rare in small animals). Pulmonary fibrosis and chronic obstructive pulmonary disease are among some of these causes where it can be severe enough to cause V/Q mismatch and, therefore, decreased PaO2.
PaO2 to FiO2 ratio
One way to determine the adequacy of oxygenation is by looking at the PaO2 to FiO2 ratio.
FiO2 represents the percentage of the oxygen the patient is breathing. Room air is 21% oxygen, so the FiO2 is 0.21. PaO2 is normally about five times that of FiO2; therefore, the normal PaO2 of a patient with no pulmonary disease breathing room air should be about 100mmHg (5 × 21%).
A normal PaO2 to FiO2 ratio is between 300 and 500. A number lower than 200 implies significant pulmonary disease or, possibly, acute respiratory distress syndrome. This ratio is particularly important in assessing patients requiring supplemental oxygen. An example is a congestive heart failure patient on bilateral nasal oxygen line (approximately FiO2 of 40%), with a PaO2 value of 80mmHg. The PaO2 appears to be adequate until the ratio is calculated (80/0.4 = 200). The change in FiO2 ratio is often more important than the PaO2 as a lone value.
A-a gradient
Once hypoxia has been established, the A-a gradient will help determine whether it is caused by ventilation failure or an underlying pulmonary disease. “A” stands for alveoli and “a” stands for arterial concentration of oxygen.
A = [FiO2 × (Pb-PH20)] – (PaCO2/0.8) – Pb is the barometric pressure (760mmHg at sea level), and PH20 is saturated water vapour pressure, which is 50. The 0.8 is the respiratory quotient and affixed number.
The simplified formula assumes the patients are breathing room air (FiO2 of 0.21) and at sea level, and the formula can be simplified to: A = 150 – (PaCO2/0.8)
A normal A-a gradient should be less than 15. Abnormally high values indicate pulmonary parenchymal disease or an underlying heart disease, while a normal A-a gradient indicates the cause of hypoxia is likely secondary to ventilation failure.
The ‘120 rule’
Ventilation is particularly important to assess in animals with respiratory compromise, as it represents the entire mechanics of breathing.
PCO2 is not only representative of the efficiency of ventilation, but also cellular metabolism and perfusion. Low PCO2, or hyperventilation, is rarely of any significance as aforementioned in the respiratory alkalosis section. High PCO2, however, is indicative of the lungs’ reduced ability to adequately shift air and can be caused by neurologic diseases, spinal cord injury, upper airway disease, trauma to the thoracic wall or muscles, and drugs that can cause respiratory depression.
Ventilation must be assessed in light of oxygenation, as both are often affected by each other. An example of this would be a hypoxic animal (low PaO2) with a compensatory hyperventilation (low PCO2). The “120 rule” will help determine whether lung function is adequate.
If the value you get, by adding the PaO2 and PaCO2, is greater or equal to 120, lung function is adequate. If the value is lower than or equal to 120, lung function is abnormal. This can only be calculated from patients breathing room air and at sea level.
Ventilation adequacy
Aside from looking at values on a blood gas, it is equally important to monitor the patient to determine whether the ventilation effort is sustainable.
Animals with a significantly increased respiratory effort – despite normal blood gas values – are at risk of respiratory exhaustion and indicative of mechanical ventilation intervention.
From these respiratory components of the blood gas value, clinicians should be able to determine the adequacy of ventilation, whether hypoxia is present and, if it is, whether the underlying cause is a result of ventilation failure or a possible underlying pulmonary or heart disease.
Once oxygen supplementation has been implanted, the PaO2 to FiO2 ratio will help clinicians decide whether the response is adequate or mechanical ventilation is required.
As with all laboratory measurements, it is extremely important to assess the patient itself. Non-sustainable respiratory efforts, in the face of normal blood gas parameters, is still an indication for mechanical ventilation.
From the moment you decide to become a vet, the road before you – from the start to the end of your course – is paved with decisions.
From where to go, to what to look for in a job (although vet students do get to put off the dreaded entrance into the “real world” for a couple more years than the average student), the next choice to be made is always around the corner.
Where to study
When it comes to picking the right veterinary degree, my opinion (which is by no means gospel) is that it’s:
10% course content
90% location, location, location
For students having a tough time choosing where to attend vet school (although, understandably, most are happy to go anywhere they receive an offer), it can be important to look above and beyond the curriculum. After all, the veterinary course in the UK is heavily standardised and, as much as every school wants you to believe that theirs has something special that nobody else’s does (and maybe they do), at the end of the day, you will leave each university with the same qualifications.
I’m not studying where I am today because I fell in love with Bristol vet school, I fell in love with Bristol itself.
I still remember getting off the coach with my dad for an open day and having the biggest smile on my face from the moment I stepped on to the cobbled streets. To this day, I’ve no idea why – perhaps it’s the multi-coloured Balamory-esque buildings, or the accents and calls of “my lover” that made me feel like I’d stumbled into a remake of Hot Fuzz, or maybe it’s the fact there are sheep and cows roaming just a stone’s throw away from the clinical campus.
Whatever it was, it wasn’t the labs, the course brochures or the lecture theatres…
For some, staying closer to home is what’s important; maybe for childcare, financial or emotional support. For others, moving away from what is familiar and stepping out of your comfort zone can play a vital part in learning independence and gaining a wider perspective.
What to study
Selective/elective weeks, while only making up a small component of your final year, are a rare opportunity to tailor your education in what is otherwise a very nationally homogenised learning infrastructure.
Work experience is another excellent outlet through which vet students can customise their teaching opportunities and prioritise what is most important to them. Practices where we feel most immediately at home are the ones that reflect our values around the profession, and the teams and individuals we bounce off easily are often indicative of the type of professional that you would/aspire to be.
Where to work
With the average retention of a veterinary professional standing depressingly at just seven short years, there’s been a massive drive from the ground up to improve the quality of the profession, and to make the career more mentally and emotionally sustainable.
We’re taught about developing resilience and mindfulness from the first year of vet school, and in the past half-decade, four-day weeks have become the standard for a lot of vets up and down the country.
With vets in such high demand, new graduates currently have a plethora of jobs to choose from. Considerations over commute times, staff retention, caseloads, OOH work, and weekend rotas (let alone salaries) are now luxuries that are becoming more and more affordable.
I would personally love to see a day when vet students can take modules in their final year – and with mixed practices decreasing in number, there may eventually be separate institutions for small animal and large animal vets.
As somebody soon to be entering the job market, I can tell you that decision paralysis is most certainly real, but I still believe that the more choices we are able to make, and the more control we have over our careers, will make us better and happier professionals.
Simple acid-base disorders are compensated by predictable compensatory changes. The primary disorder shifts the pH, while the compensatory mechanisms aim to normalise the pH and bring it back to neutral.
This is achieved by attempting to normalise the bicarbonate (HCO3-) to partial pressure of CO2 (PCO2) ratio in a paralleled manner.
For example, an increase in HCO3– (metabolic alkalosis) is compensated by an increase in PCO2 (respiratory acidosis). Similarly, a respiratory alkalosis (decrease in PCO2) is compensated by a metabolic acidosis (decrease in HCO3-).
Ruling out secondary process
However, before jumping to the conclusion an opposing change is the result of compensation, we must rule out the presence of a secondary process. This can only be determined by calculation (Table 1).
Table 1. Calculating compensatory change
Component
Expected compensation
Metabolic acidosis
↓HCO3 (↓BE)
per 1mEq/L ↓ in HCO3 = ↓ PCO2 of 0.7mmHg
Metabolic alkalosis
↑HCO3 (↑BE)
per 1mEq/L ↑ in HCO3 = ↑ PCO2 of 0.7mmHg
Respiratory acidosis (acute)
↑PCO2
per 1mmHg ↑ PCO2 = ↑ 0.15mEq/L HCO3
Respiratory acidosis (chronic)
↑PCO2
per 1mmHg ↑ PCO2 = ↑ 0.35mEq/L HCO3
Respiratory alkalosis (acute)
↓PCO2
per 1mmHg ↓ PCO2 = ↓ 0.25mEq/L HCO3
Respiratory alkalosis (chronic)
↓PCO2
per 1mmHg ↓ PCO2 = ↓ 0.55mEq/L HCO3
By comparing the reported to what the calculated compensatory change should be, you can determine whether the patient’s reported value is due to compensation or a separate disorder – for example, multiple primary acid-base disorders (a mixed acid-base disorder).
An example of a mixed disturbance could be a hyperventilating (respiratory alkalosis) dog with renal failure (metabolic acidosis).
The level of decrease in PCO2 change is in excess of the calculated compensation for the metabolic acidosis, therefore confirming a mixed acid-base disturbance. In fact, the most common causes of hyperventilation – pain, fear and excitement – often complicate blood gas analysis.
Another example of a mixed disorder could be a patient with traumatic haemothorax experiencing both lactic acidosis (hypoperfusion) and hypoventilation (respiratory acidosis) due to pleural space disease.
Waiting game
Another thing to keep in mind is compensation takes time – respiratory processes take approximately 8 to 12 hours, while metabolic processes take one to three days.
The lungs are able to alter PCO2 levels relatively quickly by adjusting the rate of ventilation. The kidneys, on the other hand, take a longer time to adjust the pH, as the change in rate of absorption and excretion of HCO3– takes much longer in comparison.
Regardless of the rate, physiologic compensation for a primary acid-base disturbance is almost never able to return pH to neutral.
Summary
A simple acid-base disorder should be suspected when the patient’s reported values are similar to the calculated compensation value, and a mixed acid-base disorder when the values fall outside the calculated range.
Another hint that a mixed acid-base disturbance is present is if the pH falls within the normal reference range, but the HCO3– or the PCO2 are not; or if the HCO3– and PCO2 are in opposite directions as opposed to being parallel.
Remember, the body can never overcompensate nor return the pH to neutral.
Base excess (BE) and bicarbonate (HCO3-) represent the metabolic components of the acid base equation.In general, both components will change in the same direction.
Decreased HCO3– and BE indicate either a primary metabolic acidosis or a metabolic compensation for a chronic respiratory alkalosis. Elevated HCO3– and BE indicate either a primary metabolic alkalosis or a metabolic compensation for a chronic respiratory acidosis.
The exception to this rule arises when a patient hypoventilates or hyperventilates.
Carbonic acid equation
CO2 + H2O ↔ H2CO3 ↔ HCO3– + H+
When a patient hypoventilates, CO2 will increase as a result of reduced expiration, so a shift to the right of the equilibrium will occur. The shift to the right will increase the bicarbonate levels proportional to the increase in CO2.
The opposite occurs when a patient hyperventilates; the equilibrium shifts to the left, so a decrease in HCO3– is present.
Since HCO3– is not independent to the patient’s respiratory status, it is an inaccurate way of measuring the metabolic component in patients with respiratory changes. For this reason, the BE value is the preferred.
The BE represents the amount of acid, or base, needed to titrate 1L of the blood sample until the pH reaches exactly 7.4, with the assumption the blood sample is equilibrated to a partial pressure of CO2 of 40mmHg (the middle of the reference range) and the patient’s body temperature is normal.
Possible causes
The possible causes of the primary disease are:
Metabolic acidosis
lactic acidosis – shock and poor perfusion
renal failure – reduced hydrogen ion (H+) excretion and increased loss of HCO3–
diabetic ketoacidosis – ketone acids
gastrointestinal (GI) losses – loss of HCO3– through vomiting and diarrhoea
Metabolic alkalosis
GI outflow obstructions – loss of H+ and chloride via vomiting
reduced chloride levels and resultant poor perfusion – body attempts to reabsorb water and sodium to increase intravascular volume, but inadvertently also reabsorbs HCO3– in the process, despite existing alkalosis
refeeding syndrome
severe hypokalaemia:
transcellular shift – potassium ions leave and H+ ions enter the cell
transcellular shift in cells of proximal tubules → intracellular acidosis → promotes ammonium production and excretion
H+ excretion in the proximal and distal tubules increases → further reabsorption of HCO3– and net acid excretion
renal insufficiency
diuretic therapy (contraction alkalosis – loss of bodily fluids that do not contain HCO3-; this causes the extracellular volume to contract around a fixed quantity of HCO3-, resulting in a rise in the concentration of HCO3– without an actual increase in HCO3– levels)
Next step
After ruling out the differential causes of either respiratory or metabolic acidosis/alkalosis, the next step is to determine whether a compensatory response is present and, if so, if this is adequate or whether a true mixed acid-base disorder exists.