Capillaria aerophila by Lalošević, V., Lalošević, D., Čapo, I., Simin, V., Galfi, A. & Traversa, D. [CC-BY-2.0], via Wikimedia CommonsCapillaria aerophila and Aelurostrongylus abstrusus are two of those most commonly found lungworm in cats.
Cats become infected with lungworm when they drink water or eat prey infected with the larval stage of the worm.
The larvae migrate out of the intestines via the bloodstream to the lungs, where they develop into adult worms and lay eggs in the host’s lungs within 40 days. The eggs are then coughed up by the cat or passed in faeces, which may then be eaten by birds, rodents and/or snails.
Symptoms include coughing, dyspnoea and mucus accumulation.
Treatment options include fenbendazole, albendazole, ivermectin, praziquante and levamisole. Usually, a 10-day course of fenbendazole with three to four days of ivermectin will clear the infection.
Coming from the centre of England, studying veterinary medicine in Scotland has its quirks. In my first week I was immersed in an entirely new language that had nothing to do with my choice of course.
One of my Scottish friends loves to remind me of the golden moment in an introductory lecture when I leaned over and whispered “who’s Ken?” (as in “I dinnae ken”, or “ken what I mean?”).
But this week, during a lecture on bovine viral diarrhoea (BVD), I was left wondering about the geographical impact of studying in Glasgow compared to friends who stayed closer to home.
North of the border
The BVD virus has a pretty interesting mechanism that, while making for fascinating reading, is the reason it wreaks havoc on the UK’s cattle industries and can be pesky to both diagnose and get on top of in the herd.
While BVD is prevalent all over the UK, Scotland is significantly further ahead than my home turf in the control of this disease, mainly due to a government-implemented eradication programme in recent years.
In England, however, many farmers are unaware of the disease or reluctant to undertake the costly exercise of hunting persistently infected calves within the herd, which, at the moment, is not compulsory – unlike in Scotland.
Now there was a lot of joking about England letting the side down and being a bit useless, but the reality is that until England plays catch-up and implements an eradication scheme, it’s going to be extremely difficult for the Scottish eradication to be 100% successful – short of throwing up a double fence between us and them.
Regional issues
If I were studying elsewhere, I wonder how the emphasis would differ depending on the prevalence in that region. Several times in my lectures I’ve heard Angiostrongylus (heartworm) brushed off as a differential if the animal has been to the south of England, with little much else said.
Would that be given more time in an area with higher prevalence, if I were studying in London for example?
At the end of the day, we all come out as vets, no matter where we’ve studied, and, while some topics may get more emphasis because of their regional importance, we’ll still need to pay particular attention to those conditions or diseases more commonly found in the areas we end up working in. So I don’t think geography has a dramatic impact long term (unless you never intend to leave your university city).
Hold the stomach tube against the plastron of the tortoise with the tip at the caudal end of the abdominal shield.
Make a mark on the tube just cranial to the jugular notch.
Sit the tortoise upright on its tail and hold the head out of the shell with the middle finger and thumb on each side of the neck. This will extend the oesophagus.
Open the mouth, using the forefinger to prevent the tortoise closing it again.
Lubricate the stomach tube (KY is fine) and press the tip through the mouth and over the back of the throat. It should slip down easily and you may feel the tip passing through the cardiac sphincter. Stop when the mark on the tube enters the tortoise’s mouth.
Resolution of the hypovolaemia is the primary concern. Two large bore catheters are placed in the cephalic veins. If the cephalic veins are not available, the jugular vein is used. Fluid resuscitation through the saphenous veins is unlikely to be successful because of the caudal vena caval obstruction.
Photo of an x-ray showing gastric dilatation and volvulus in a large mixed-breed dog. The large dark area is the gas trapped in the stomach. The pylorus and duodenum are in an abnormal position cranial to the stomach and are separated by a fold in the stomach, creating a “double bubble” appearance.
Image by Joel Mills [CC-BY-SA-3.0], via Wikimedia Commons.Either isotonic crystalloids (90ml/kg in the first hour) or hypertonic saline (7% NaCl in 6% Dextran: 5 ml/kg given over five minutes) followed by crystalloid are administered.
Controversial treatments
The use of corticosteroids remains controversial. They have many theoretical benefits but have not been unequivocally demonstrated to improve survival in cases of gastric dilatation-volvulus (GDV).
Prophylactic antibiotics are also somewhat controversial, but rational arguments are made for their use. GDV dogs do have increased levels of circulating endotoxin, perhaps indicating increased GI mucosal permeability. Poor perfusion to the liver could inhibit reticuloendothelial function.
Improving tissue perfusion by fluid resuscitation and subsequent gastric decompression and de-rotation can potentially result in the production of damaging, highly reactive oxygen free radicals. These radicals can cause significant reperfusion injury that may be as damaging as the initial hypoperfusion episode.
It is possible treatment to prevent free radical generation may be beneficial in dogs with GDV. Of the drugs trialled in experimental models, deferoxamine, an iron chelator, shows the most promise for clinical application.
Gastric decompression
Ideally, a continuous electrocardiogram is connected. Once the animal has been stabilised, gastric decompression is attempted using a silicone or rubber tube. The tube is pre-measured to the level of the stomach and marked. A 2in roll of tape is placed in the dog’s mouth and the tube passed through the tape and slowly into the oesophagus and stomach.
If resistance is encountered at the level of the cranial oesophageal sphincter, the tube must not be forced, as this could cause rupture of the caudal oesophagus.
In some fractious animals, sedation and intubation is necessary for gastric decompression. If orogastric intubation is unsuccessful, the stomach is decompressed by trocarization. The abdomen is carefully palpated, and the enlarged spleen is avoided. A large gauge catheter (10-12F) is placed into the stomach percutaneously to relieve pressure.
Currently nursing a bruised tailbone after being propelled twice from a four-legged fiend I had a disagreement with regarding a small upright jump, I can’t help but wonder why we do these stupid things.
Horses can be hazardous enough when you’re on top of them, but they’re not all angels at ground level either. The results of a 2014 study commissioned by BEVA revealed equine vets are at the highest risk of sustaining injury out of all the civilian occupations in the UK.
While these results have been published for some time, and whether the news was surprising or not on first reading, my recent injury certainly made me consider more seriously whether we are cautious enough around horses in a veterinary context.
I was probably about as safe as possible this week during my falls, kitted out with a high standard helmet and air jacket, yet I still got injured. We can’t prevent every injury or accident possible, but we can try to take measures to minimise the damage.
The second most common site of injury reported by equine vets in the study was the head, but when was the last time I saw a vet enter a stable wearing any form of head protection? Never.
In some cases, I believe this is a matter of pride, practicality or even client confidence. If a vet turned up at the yard with a riding hat on, clients may believe they’re not confident around horses – and how difficult is it to look into a horse’s mouth while rasping teeth with bulky headgear?
“Jousting? No, I’m just off to the stables…”
However, safety should come first and perhaps vets should consider being more vigilant, despite the potential judgemental attitude they may be presented with.
What about repro work? I’ve seen many a fractious thoroughbred mare lash out with her hindlegs while being scanned, luckily with an appropriate board or stocks used to protect the vet. But I have seen an equal number of occasions when vets have been rectal scanning with nothing except confidence in a “good tempered” horse to protect them.
So, how can we make situations like that safer, short of carrying a portable kick board in the car or persuading clients to invest in appropriate equipment.
It should be a daunting prospect entering a profession that has been proven to carry the highest risk of injury in the country, and yet most of us take this as a given, not giving it much thought. The results of the study have only confirmed what many of us already knew about equine work, but I think it should act as a wake-up call to encourage vets or practices to alter policies to maximise safety in the field.
After all, it would be pretty miserable work if most of the time was spent hobbling around like I currently am.
Syringomyelia is rare in most dog breeds but has become widespread in cavalier King Charles spaniels.
Syringomyelia is a condition where fluid filled cavities develop within the spinal cord. It is sometimes known as “neck scratcher’s disease” because scratching in the air near the neck is a common sign.
Owners often report their dog is worse at night, when first getting up, during hot or cold temperature extremes, when excited, or related to posture (e.g. preferring to sleep with their head elevated).
Affected animals may seem overly sensitive to touch, or to scratch more on one side of the neck, ear, shoulder or sternum. This is typically one side only, often while the dog is moving and sometimes without making skin contact. Some dogs, especially younger patients, develop a scoliosis.
Some severe cases may have other neurological deficits such as fore and hind limb limb weakness and ataxia.
Facial nerve paralysis, deafness and seizures have also been associated with the condition, but a link has yet to be proven.
Reptiles, being cold blooded, are dependent on the environment to provide sufficient heat. If they get cold, their metabolism can become so sluggish that they cannot defend themselves, not even against a mouse.
Careless owners of small snakes have been known to toss a live mouse in with the snake and then not supervise. If the snake is cold, the mouse can eat the snake alive and the snake cannot retaliate.
If the snake survives such an attack, it may have such a fear of mice that it will no longer eat. It can take a year of tube feeding before the snake gains the confidence to face another mouse.
I’m a bit of a grammar Nazi, so getting involved in editing has been a lot of fun.
I enjoy writing about my experiences, but I also enjoy reading about others. I’m also a bit (or a lot) of a grammar Nazi, so getting involved in editing over the past couple of years at university has been a lot of fun.
I started by subediting the University of Glasgow’s student newspaper and proofreading emails/letters for fellow students on the organising committee for a charity event, before taking on the role of editor for the student vet magazine (JAVS), which goes out to all UK veterinary schools.
This is something I love doing, but it does have its downsides – and it sometimes feels like trying to draw blood from a stone. The past few editions of JAVS have seen a serious deficiency of contributors, but each one has been saved by my persistent chasing of articles, rallying people I know have an interesting story to tell, and reassuring those who’ve been asked to write but lack confidence in their ability.
Now this begs the question: why do veterinary students not want to write?
Are they too busy and see it as pointless extra work that won’t be recognised or count towards their degree?
Are they worried about not producing an item good enough to publish?
Do they lack confidence in their linguistic abilities?
While the vet degree is insanely busy and students will count every precious moment of free time they have, there are considerable advantages to having a piece of writing published – be that in print or on the internet.
Getting your name out there
“Writing for a student publication is a great start in order to get into the swing of things without strict word counts or other constraints.”
It’s surprising how far an article or blog post can reach. People with seemingly nothing to do with the veterinary profession or, alternatively, those higher up in the profession may see them.
Social media provides a particularly excellent platform for getting your work out there – many of the student written articles published on the AVS (Association of Veterinary Students) Facebook page have received “likes” or comments from BVA and RCVS presidents.
For those looking to publish in the future, whether through research or journalism, writing for a student publication is a great start in order to get into the swing of things without strict word counts or other constraints.
Even if you have no interest in writing as part of your career, having your name on an article can have other advantages. Who knows, maybe in a few years your future employer may have been intrigued by something you’d had published – which could make the difference between being asked to interview or not.
Spread the word
Sharing ideas with other students allows writers the opportunity to pass on information that could benefit other parties as well. For example, if someone undertakes EMS with a charity he or she feels is a particularly worthwhile cause and needs extra help, writing an article to raise awareness could give the organisation a huge boost. It will also make fellow students aware so they could go and have the same great experience as others before them.
Even sharing hints and tips for other things vet related might help other students avoid common mistakes or guide them more smoothly through the maze of the veterinary degree.
Don’t be scared
“Don’t be scared. Bite the bullet. Put pen to paper (or fingers to keyboard) and just go for it,” says Jordan.
It has been suggested many veterinary students don’t want to write because they don’t think they have anything interesting to say, or worry their finished piece won’t be good enough for publication – and I appreciate writing doesn’t come naturally to everyone, but that’s where I come in.
I can’t magic up the entire content for a whole magazine, but if students give me some ideas to work with – regardless of how scrambled they may be – they can be edited into fully formed articles.
It may be that self confidence is the issue, but don’t worry, everyone has to start somewhere. Your first attempt wont necessarily be the next Harry Potter phenomenon, but I guarantee that most veterinary students do have interesting experiences or ideas to talk about – so don’t be scared. Bite the bullet. Put pen to paper (or fingers to keyboard) and just go for it.
Getting published can open a lot of doors you didn’t even know were there, so I would encourage every veterinary student to try to get their names out there. After all, the veterinary world is smaller than you think, and you never know who might be reading.
A histiocytoma on the ear of a boxer dog. Image by Joel Mills (own work) [GFDL, CC-BY-SA-3.0 or CC-BY-SA-2.5-2.0-1.0], via Wikimedia Commons.Histiocytomas are common, benign skin tumours that begin in the immune cells. They usually present as small, firm, dome or button-shaped masses on the skin surface, which are fast growing, non-painful, and usually solitary.
Common sites include the head, nose, ear edges, and limbs. Occasionally, multiple skin nodules or plaques are present. Rarely, an autoimmune blistering is possible that may ulcerate.
Histiocytomas can also occur internally – in the stomach, lungs and intestines.
Retrievers, bull terriers, cocker spaniels, and great Danes are more susceptible to histiocytomas. The masses often spontaneously regress over two to three months.
The most common problem that arise from histiocytomas is when they become pruritic, triggering self-excoriation and infection. Excision is then required.
Anorexia in rabbits is a medical emergency and should be treated aggressively.
Anorexia in rabbits is a medical emergency and should be treated aggressively.
Subcutaneous, intraperitoneal or intraosseous warm isotonic fluids given several times daily will improve hydration and help stabilise the rabbit. Fluids can be given using a 20 or 22 gauge needle into the medullary cavity of the femur.
Syringe feeding nutritious high fibre slurry will increase nutritional status, help prevent ileus and rehydrate stomach contents.
Commercial products such as Critical Care, or homemade diets – such as yoghurt mixed with pureed vegetables, ground feed and glucose solution or baby pablum with a small amount of psyllium fibre and probiotic powder – have also been used successfully.






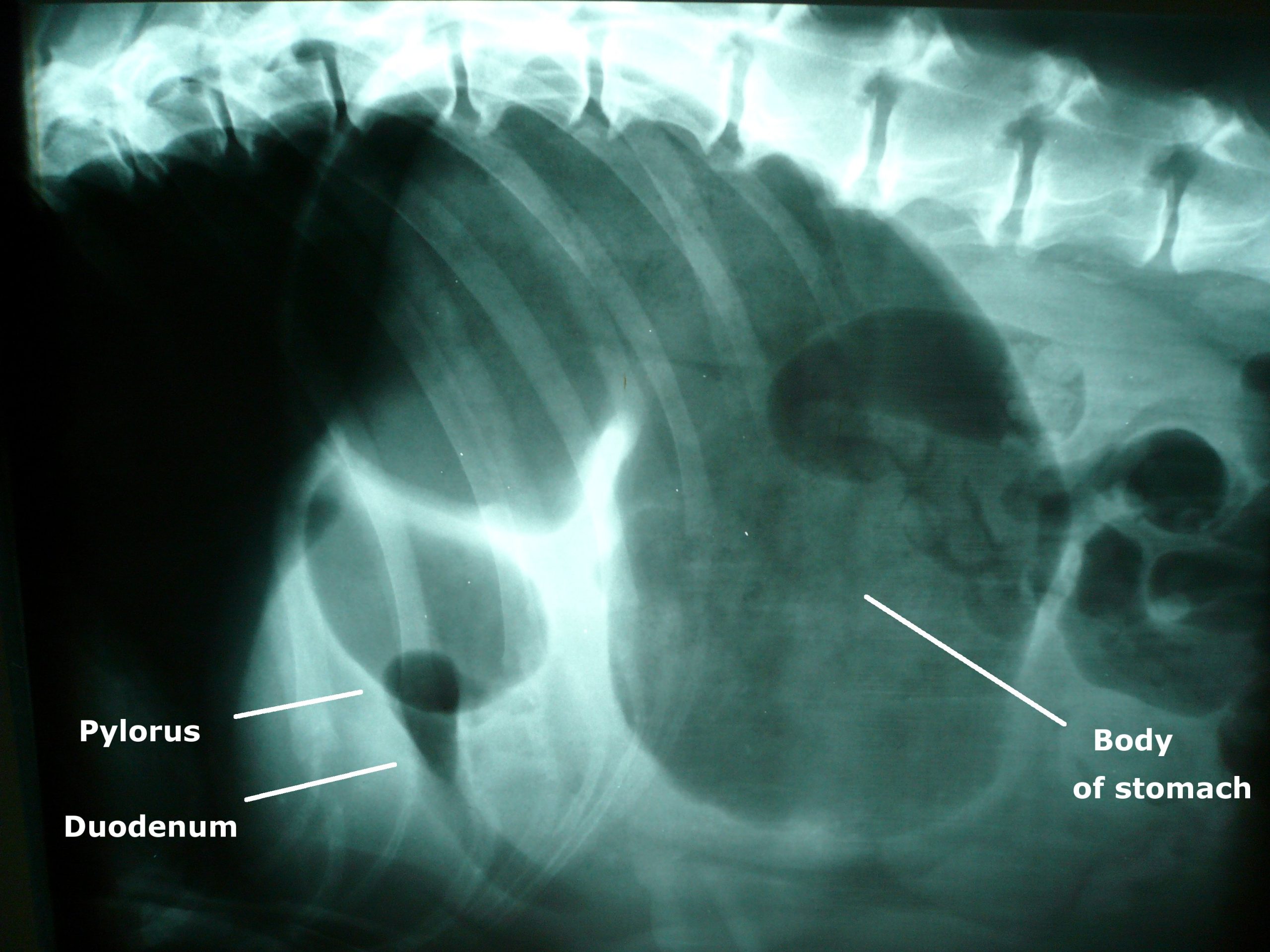
![Photo of an x-ray showing gastric dilatation and volvulus in a large mixed-breed dog. The large dark area is the gas trapped in the stomach. The pylorus and duodenum are in an abnormal position cranial to the stomach and are separated by a fold in the stomach, creating a "double bubble" appearance. By Joel Mills (Own work) [GFDL (http://www.gnu.org/copyleft/fdl.html), CC-BY-SA-3.0 (http://creativecommons.org/licenses/by-sa/3.0/) or CC-BY-SA-2.5-2.0-1.0 (http://creativecommons.org/licenses/by-sa/2.5-2.0-1.0)], via Wikimedia Commons](http://www.vettimes.co.uk/app/uploads/2013/09/GDV_x-ray.jpg)












{kind=link}