Pulse oximetry is a very useful diagnostic and monitoring tool that has become commonplace in veterinary clinics. It measures the percentage of haemoglobin saturated with oxygen, and is an indirect measure of arterial oxygen levels.
Dog with pulse oximetry.
However, here are several important points to help you understand the limitations of pulse oximetry.
Causes for false readings
Falsely low readings:
motion artefact
peripheral vasoconstriction/low tissue perfusion from hypothermia or shock
pigmentation of mucous membranes
thick hair coat
Falsely high readings:
haemoglobin abnormalities (carboxyhaemoglobin and methaemoglobin, for example)
False sense of security
Pulse oximetry can give us a false sense of security. We hold on to the adage “95% and above means everything is going along swimmingly”, but that couldn’t be further from the truth:
Pulse oximetry can give us a false sense of security.
It does not detect hypoventilation or apnoea: it can take several minutes for apnoea to result in hypoxaemia that is detected on pulse oximetry; therefore, it cannot be used as a sole measure of respiratory adequacy. This is best measured by capnography.
A common misconception is the oxygen saturation will drop with patients with anaemia. This is incorrect. The haemoglobin present in the decreased number of red blood cells will still be saturated to normal levels. However, this cannot be interpreted as the patient having adequate oxygen delivery to its tissues.
One last point: due to the oxyhaemoglobin dissociation curve, any drop below 94-95% is significant and warrants investigation. At 95% SpO2 the partial pressure of oxygen in the arterial blood is 80mmHg (normal), but at 90% SpO2 the partial pressure is 60mmHg (severe hypoxaemia) – for only a small percentage decrease, there is an exponential reduction in arterial oxygen content. This is even more important when patients are receiving oxygen therapy as the patient’s SpO2 should be 99-100% normally. So when a patient has an SpO2 of 95%, but is on high rates of oxygen, then significant respiratory compromise/disease must be present for an SpO2 of 95% or lower to occur.
For some, my past A-level choices of biology, chemistry and English literature may seem an odd mixture.
At first glance, the arts and the sciences don’t seem go hand in hand, and are often viewed as polar opposites. I even remember being asked during one of my veterinary interviews if my decision to study English lit was an indication that I valued the arts above the sciences…
As someone who had endured a considerable wealth of hours endeavouring to make it into vet school (and was, in fact, at an interview for vet school), it took me a couple of blinks before I could bring myself to answer that question.
Words, words, words
Since then, I am still yet to find another vet student or graduated vet who took English as their third A-level choice – perhaps because, until recently, most vet schools wouldn’t accept anything other than physics, maths or maybe economics at a push.
With three years of the vet course down, and a master’s dissertation currently weighing on my shoulders, this truly baffles me, given that writing is such an inherent part of the scientific process.
Whether it’s animal welfare, physiology, psychology or behaviour, almost everything we know and practice today can be attributed to some budding young scientist who did the research, wrote it up very eloquently, and had other scientists read over it diligently before they decided to write about it, too (otherwise known as a peer review).
Similar principles
Today, it does not matter how big of a breakthrough you make; if your grammar isn’t on point, nobody is going to publish it and your discovery may well fall on deaf ears. If you don’t know at least five different words for “furthermore” and can’t tell your colons from your semi-colons then are you even a scientist?
I have personally always loved writing (couldn’t you tell?) and being able to combine my affinities for that with veterinary medicine sometimes feels a bit too good to be true.
I also feel incredibly grateful for the skills my background in English have taught me. I may no longer be comparing the works of Mary Shelley and Thomas Hardy, but strangely, the same principles can be applied to literature reviews and grant proposals.
Do what you love
I would strongly encourage any wannabe vets not to shy away from exploring interests outside of the sciences, if that’s what you really enjoy.
For me, an artier A-level was a really useful way to switch off the science part of my brain and recharge after a day of balancing equations – almost like my right and left brain taking turns at the wheel while the other had a little lie down.
And who knows, if more medical schools required an A at English A-level, doctors might be know for better handwriting.
We’ve all heard horror stories of dogs left in hot cars by their owners; it’s an issue that comes around every year like the warnings of dangers of chocolate at Easter and mistletoe in December.
Luckily, I’ve never seen a case brought into practice or even witnessed a dog shut into a car on a hot day – until this week.
While shopping, I noticed a small Westie lying rather forlornly in the back of a parked car. The windows were cracked and it was a cloudy day, so the owners had obviously assumed popping into the shop for however long they’d intended would do their animal no harm. Not surprisingly, I was immediately concerned.
Getting hotter
Despite the clouds it was a hot day and muggy – and as it was only 11 in the morning, the temperature was only going to rise. No water had been left for the dog (either out of laziness or for fear that it would be knocked over), and although I could tell he was alert, he moved from seat to seat, clearly agitated and anxious.
I’d hope the average passer-by would intercede, but being a veterinary student with all the worst-case scenarios scarred permanently into my brain, I didn’t feel right leaving it.
The situation didn’t seem urgent enough to warrant bashing the windows in – especially as I had no idea if the owner was just around the corner. Instead, I checked with the shop the car park belonged to, and although it didn’t have a tannoy system they thanked me, took down the registration number of the car in question and promised to watch diligently until the owner returned.
Legislation lacking
Since then I have been brushing up the laws in the UK regarding leaving animals in cars, and although it is not illegal to leave a dog in a car (regardless of the temperature, or the windows being rolled up or down), the owner may be prosecuted if anything happens to the animal in that car.
Given the number of dogs that die in hot cars, or shortly after being left in one every year, I think that this legislation needs to be reviewed. If you wouldn’t leave a child in a car unattended, why leave an animal that is arguably even more vulnerable?
What to do?
For anyone who finds themselves in the position I was – and there’s nobody around to help, the animal seems distressed or in danger, or you simply don’t know what to do – please know you are absolutely within your rights to call 999 and contact the emergency services. The best case scenario will be that the animal is absolutely fine and no intervention is needed – the worst case scenario is far, far worse.
Try to check how long the car has been there by looking for parking tickets. If you’re unsure whether a dog is suffering within a hot car, look for signs of heatstroke/hyperthermia such as heavy panting or drooling, lethargy, collapse or vomiting.
More advice can be found on the RSPCA or PDSA websites, and if in doubt, the RSPCA hotline (0300 1234 999) is available for advice.
Blood smear evaluation is an often overlooked, but very important, aspect of an in-house haematology.
With the advancement in haematology analysers that can now detect reticulocytes and even band neutrophils, some practitioners are beginning to rely solely on the numerical data alone in evaluating the patient’s blood.
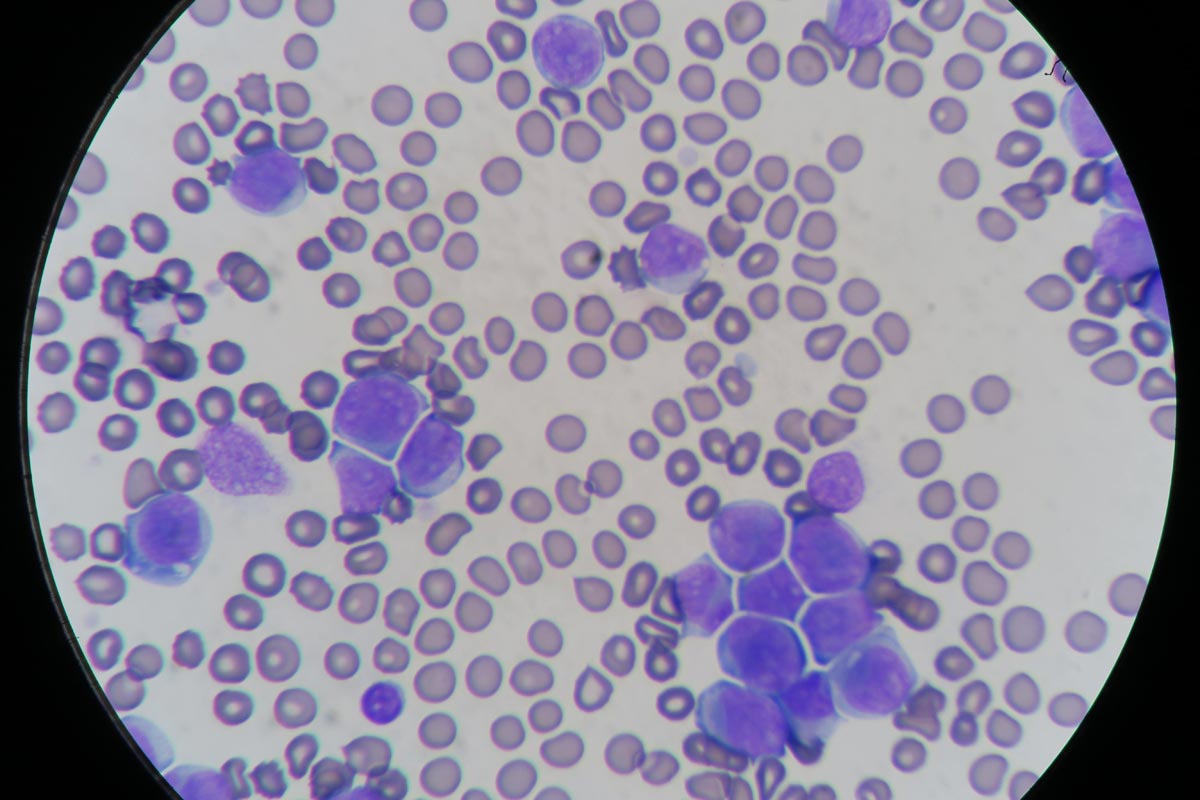
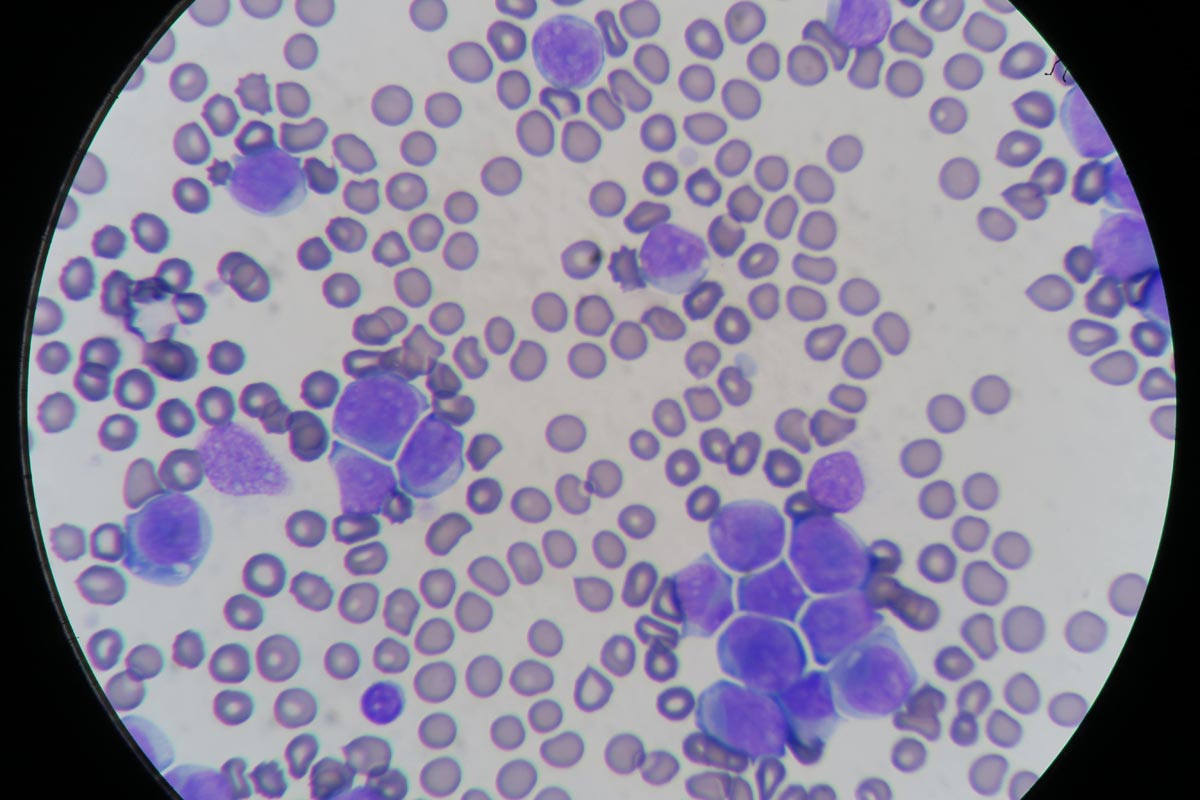
Patient with elevated white blood cells caused by leukaemia (click to zoom).
The art of blood smear interpretation is on the decline. However, it is an extremely valuable skill that must be practised and perfected and really should be part of every in-house haematology.
Plus points
What are the benefits of being good at blood smears?
Identifying a regenerative response, looking for reticulocytes (polychromatophils).
Looking for other possible causes of an anaemia – such as Heinz bodies, infectious microorganisms or spherocytes, which can indicate an immune-mediated haemolytic anaemia.
Confirming thrombocytopenias, as frequently platelet clumping can be reported as a thrombocytopenia.
Assessment of the nature of a leukocytosis. High leukocyte counts do not always mean infection. Neutrophilia can be caused by both elevated immature and mature neutrophils. Determining the nature of neutrophilia can provide crucial information in identifying the underlying cause and if the patient is coping or not. Apart from infection, other causes can include stress, corticosteroids and neoplastic leukaemias.
Normal leukocyte counts do not always mean the patient is okay. Patients can have severe left shifts, but normal leukocyte counts.
Practice makes perfect
Blood smear evaluation begins with becoming accomplished at producing great diagnostic smears. This takes practice; poorly performed smears can be non-diagnostic and frustrating to assess for both yourself and an external pathologist.
A few tips on the technique:
Use a very small drop of blood. If you have picked up too much blood with the “spreader” slide, lift off and start the smear away from that drop of blood.
Angle the “spreader” slide about 30°. The bigger the angle, the shorter your smear.
Push the “spreader” slide forward.
The smear should end at about half to three-quarters of the way down the slide and must have a “feathered edge”.
Adverse events during anaesthesia in otherwise young and healthy patients is a rare occurrence. However, with low incidence of adverse events could come an increased risk of complacency on the part of the veterinary team.
Take the following case as an example:
Clicky the cat with Gerardo and his team.
“Clicky” is a young and healthy cat that underwent a routine dental prophylaxis procedure. A few days after the procedure, she developed respiratory difficulties and presented to our emergency clinic.
Possible problems
She was diagnosed as having severe subcutaneous emphysema, most likely from a tracheal wall compromise that would have occurred as an adverse event from tracheal intubation.
We need to handle cats very gently while they are intubated as their tracheas are nowhere near as robust as their canine counterparts.
Overinflating the cuff is another cause of tracheal necrosis.
Never be complacent
What we think happened was the patient was repositioned during the dental procedure and the endotracheal tube was twisted in the process, causing either ischaemic compromise to a portion of the trachea or direct damage to the trachea.
Thankfully, “Clicky” made a full recovery, but this case certainly highlights that we must never be complacent when it comes to handling our anesthesia cases.
Low incidence does not mean no incidence, and individualised anaesthetic plans – along with in-depth training for the anaesthetist (who most often are veterinary technicians and nurses) – will help reduce the chances of adverse events occurring.
Technology has changed how we practice veterinary medicine. Gone are the days of the paternalistic relationship between vet and client, where the client will simply go along with whatever the vet deems necessary for the pet.
Clients are becoming more knowledgeable and, as vets, we’re often faced with a situation where a client comes in armed with a “Dr Google” diagnosis.
As practitioners, this can be challenging and confronting – maybe because our egos tell us it is an insult to our hard-earned years of training and experience. If this is the case, I think our perspective needs to change.
Changing perspectives
Working in an emergency clinic, we regularly talk to clients with questions about something they have read on the internet. I confess I used to feel threatened by this. However, I wasn’t comfortable feeling this way, so I decided to change my perspective on the matter.
Is it time to call a truce with Dr Google?
Here are some ways to turn the old nemesis, Dr Google, into a friend – or, at the very least, call a truce:
Make it a point to acknowledge your clients for their initiative and interest in their pet’s health. You are not simply paying lip service, here – the reason these clients have searched for information about their pet’s health is because they care.
These clients are generally dedicated to their pet’s health and welfare; they are the ones who are often committed to doing what needs to be done, as long as they understand why and how – and that’s where you come in. Client education is a big part of our jobs.
They are pre-armed with knowledge, therefore saving time in the consult room, so you can spend less time describing what the adrenal glands do, for example, and more about why and how they can malfunction.
If what they have read is inaccurate, take the opportunity to gain rapport by giving them the correct information or directing them to reputable sites, such as VeterinaryPartner.com – this demonstrates to clients you are still the most reliable source for information about their pet’s health.
Genuine concern
Due to the ubiquity of information (and misinformation) about veterinary medicine available on the internet, there is an even stronger reason for us, as vets, to keep up with the latest advancements in veterinary medicine.
Always try to remember, ultimately, the reason your clients have come to see you having already done some research on the internet is because they are genuinely concerned about their pet – so try to see this as something positive, rather than negative.
By changing your perspective, you’ll soon find you no longer dread a consult with clients who have brought Dr Google along.
The assumption is often made that many people get into the veterinary industry for the money. In fact, it’s always been a widely held public view that vets are raking it in.
This is, perhaps, due to a combination of the recognised difficulty of the job, seemingly extortionate vets’ bills and a propensity for Range Rovers.
Whatever the cause, this view was made all the more apparent on the 18 May edition of Good Morning Britain.
Concerns about cost
The original topic of debate – “Should there be an NHS for pets?” – sparked a subsequent debate into the pricing of veterinary care, with strong implications being made that pricing in the veterinary industry is “unregulated” and, therefore, unnecessarily high and perhaps even greedy?
As an outsider looking in, faced with an objectionably large bill for what you thought would only be a routine check-up, I can see how it’s easy to misunderstand where all that money can go, except into the pockets of the vets themselves – and yet this is a fallacy.
Clients just don’t understand
I feel an understandable nationwide misunderstanding exists of the true value of what we consider to be “routine” medical goods and services.
According to an NHS calculator, without health care, the price of a hospital child delivery would range from £2,500 to £5,000, depending on any complications. In the US, a single doctor’s consultation can cost you upwards of $200 (£141), with the average American spending more than $10,000 (£7,000) in health care a year as of 2016.
There’s no denying that we take human medical care for granted, so there’s little surprise when the cost of animal medical care puts our clients in need of a pacemaker (free of charge).
In it for the money
One of the very first things I learned about veterinary medicine – as I sat, rather excitedly, in a school-organised lecture given by the head vet of a local practice to a room of young, naive wannabe vets – was that if we were thinking of getting into the career for the money, we should change tack now, as we would be sorely disappointed.
I know I am luckier, now than ever before, to have the luxury of both job and financial security when I leave university, but it needs to be said that neither myself, nor any vet student I have ever encountered, got into this business for the money.
Even if we had, I think it would be fair to call us fools, as there must surely be an easier way to make money than five years of student housing, student loans, exams and poop scooping.
Initial outgoings
I think it also needs to be said that the phrase “it takes money to make money” could indeed be applied very aptly to the veterinary degree. A growing awareness exists of the potential accessibility imbalance when it comes to the vet course, depending on background, social class, funding and so on.
It’s no secret to those on the inside that getting into, and through, vet school can insure some serious dents in your wallet, and those of your parents (sorry parents); between textbooks, steel toe-capped wellingtons, petrol miles, Airbnbs for long-distance placements and stethoscopes (the most expensive necklace you will ever own), you are looking at a sizeable sum before you even get to student loans.
And that’s without considering being able to afford the time off work to travel to open days and interviews in the first place, with the assumption that you have a supportive network of family who have the money to fund your ambitions before you’ve even got your foot in the door…
An NHS for pets?
The topic of an NHS for pets aside, I think a great deal needs to be done to help us recognise the true privilege that is our human NHS, and the true value of the service given by all medical professionals.
The nature of the vet course is inherently competitive, with the odds stacked against you from the very beginning.
During our A-levels we are told that only 1 out of every 5 to 10 applicants make it to vet school, and that you’re lucky to get a single interview or offer (any more than that is just greedy).
In university, when students on other courses are totalling up their grades to calculate if they are getting 1sts or 2:1s, vets are given a pass mark of 50%, which has the paradoxical effect of making it seem like you should be sailing through the course when, in actual fact, the bar is set so low because – yes – it really is that hard.
Negative feelings
The majority of vets and vet students, I am sure, can report to experiencing some form of impostor syndrome at some point in their careers – if not throughout.
Impostor syndrome is the feeling you are not as bright, or competent, or worthy of where you are in life as everyone around you thinks you are. It can be a toxic, self-deprecating and sometimes debilitating sensation, making you feel entirely alone when really everyone around you is most likely in exactly the same boat.
No motivation
From a little of my own experience, and through speaking to others in the field, I know this feeling has only grown stronger among my peers as a result of the coronavirus pandemic.
After almost a year of online learning, open book exams and, in some cases, a complete lack of the hands-on practice and subsequent reassurance we should all be receiving right now, it’s only natural things don’t feel quite right.
No motivation. Photo by Andrea Piacquadio from Pexels
Being cooped up all day, and going long periods of time without seeing friends and loved ones, certainly doesn’t inspire productivity, and it can be hard to stay motivated with nothing to look forward to on the horizon – whether that’s a long holiday in the sun or just a nice catch-up with your mates down the pub at the end of the week.
Under pressure
After a year of lockdowns with nothing else to do, I think it’s all too easy to put too much pressure on yourself to accomplish everything because, look, you’ve never had this much free time before!
I’ve heard from lots of students who think – especially due to last year’s open book exams – that they “don’t deserve to be here“; that they haven’t worked as hard as they could have, or should have; that they’ve dropped the standard, so to speak.
But that’s the thing, even if it doesn’t feel like you’re working as hard as your old self used to in “the before world of February 2020 and earlier”, that’s because this is a completely different kind of work.
Marathon effort
It’s so much easier to sit down and do a day’s work with no distractions when the rest of your life is stable, but when it’s not, even the little things can become difficult – and that’s okay.
Take marathon runners, for example: capable of running for miles and miles, so of course, that first mile, or even the first 10, probably feel like nothing (as a max 10km runner I wouldn’t know personally, but I can assume).
That 25th mile, though – when they’ve already come so far, they’re worn out and their energy reserves are entirely depleted – is probably the hardest one of all. It’s likely a challenge to just put one foot in front of the other. It’s going to feel like they’re working 1,000 times harder than they had to for that first mile, even though the distance hasn’t changed – the conditions have.
Photo by Tembela Bohle from Pexels
Third and final (?) leg
As the third lockdown trickled ever so slowly onwards, I think everyone felt like they were just trying to keep up on what they hope is going to be the last leg of this unprecedented journey.
For marathon runners at least, they know how long that run is going to be, so they can go all out on that final sprint. In lockdown terms, though, we don’t really know when this race is going to be over (despite the Government’s road map out of lockdown) – and that makes it okay to not feel like you have to give it your all every single day, but leave some in the tank so you can keep going the next day and the next.
No shame
What I’m trying to say (through some very dodgy metaphors) is that we’ve all come so far, and there is no shame in taking extra days off, or extra rest breaks; that if you passed an exam or a year at vet school – open books or not – you deserved that pass.
It was probably one of the hardest exams you ever had to take, at the dawn of a global pandemic when no one knew up from down or left from right.
We all need to be proud of ourselves for whatever we’ve achieved over the past 12 months, even if that’s just making it through and being there for each other.
In the previous post we covered what to look out for on ultrasound when assessing for a linear foreign body. Now we discuss the things you should consider before deciding to take the patient to surgery.
Read the following statements and answer the questions – either yes or no…
Linear foreign body surgeries can be technically difficult and can take a prolonged period of time to perform. The longer the surgery, the higher the rate of complications. Are you (or do you have access to) an experienced surgeon who has performed a linear foreign body surgery before, and do you have an additional pair of hands for surgery to help reduce surgery time?
Were bacteria visualised or is their presence likely based on the comparison of the abdominal fluid glucose and lactate to peripheral blood (see previous post)? If yes, then septic peritonitis is present. Approximately 40% of dogs with linear foreign bodies will have septic peritonitis. This means you need to be prepared to perform a resection and anastomosis; sometimes two. Have you performed a resection and anastomosis before?
Often a combination of gastrotomy, enterotomy, and resection and anastomosis are required. Are you prepared to perform a combination of these surgeries?
Linear foreign body surgeries can often require a significant number of surgical instruments and consumables. Do you have Balfour retractors, forceps, clamps, additional kit for closure, supply of lap sponges, as well as substantial amounts of lavage and access to suction?
Linear foreign body patients are often critically ill due to septic peritonitis. They can present in shock and have biochemical derangements such as hypoalbuminaemia, which indicates the need for perioperative critical care. Do you have experience stabilising, performing anaesthesia and postoperatively managing a critically ill patient?
Hypotension can be caused by hypovolaemia; however, if the hypotension has not responded to reasonable volumes of a balanced isotonic crystalloid fluid – for example, 30ml/kg to 40ml/kg – then the hypotension could be caused by vasodilation from septic shock. This means vasopressor agents will be required in addition to crystalloids. Do you have access and experience with vasopressor therapy?
Image: Gerardo Poli.
Conclusion
This list of questions is not meant to be conclusive or definitive, but merely a list of considerations before taking a linear foreign body patient to surgery.
If you answered no to many of these questions, then consider referral to a facility that is prepared and equipped for the challenges that often accompany linear foreign body patients. However, if referral is not an option, consider the list above as a way to be as prepared as possible for tackling those situations.
If used by an experienced ultrasonographer who knows what to look for, ultrasound can be a highly sensitive and specific diagnostic test.
What do we look for?
Remember not all patients will have intestinal dilation as the linear foreign body may be only causing a partial obstruction. Alternatively, it could be occluding the gastric outflow completely.
Intestinal plication, which looks like intestinal loops bunching up on each other around the tether.
A central discrete hyperechoic line running along the middle of the bunching intestine. This bright line is the tether. Often when looking closely enough, the tether will have distal acoustic shadowing as the ultrasound pulses cannot pass through it.
The leading aboral segment and the trailing adoral anchor will have acoustic shadowing.
The adjacent mesentery is often hyperechoic compared to other areas in the abdomen, indicating inflammation.
Gastric dilation with fluid is often seen if the anchor is in the pylorus, as it causes an outflow obstruction.
Free abdominal fluid may be visible and a sample should be collected for assessment. If bacteria can be demonstrated in one of the following ways:
By visualising free or intracellular bacteria under the microscope.
By finding that the glucose is lower (lower than 20mg/dL) and the lactate is higher (2mmol/L) in the abdominal fluid sample compared to peripheral blood then this indicates perforation of the gastrointestinal tract has occurred and septic peritonitis is present.
In the third and final post, we will cover things to consider when deciding whether to perform the exploratory laparotomy yourself, or if you should transfer the patient to a referral facility for surgery.









 Technology has changed how we practice veterinary medicine. Gone are the days of the paternalistic relationship between vet and client, where the client will simply go along with whatever the vet deems necessary for the pet.
Technology has changed how we practice veterinary medicine. Gone are the days of the paternalistic relationship between vet and client, where the client will simply go along with whatever the vet deems necessary for the pet. 






