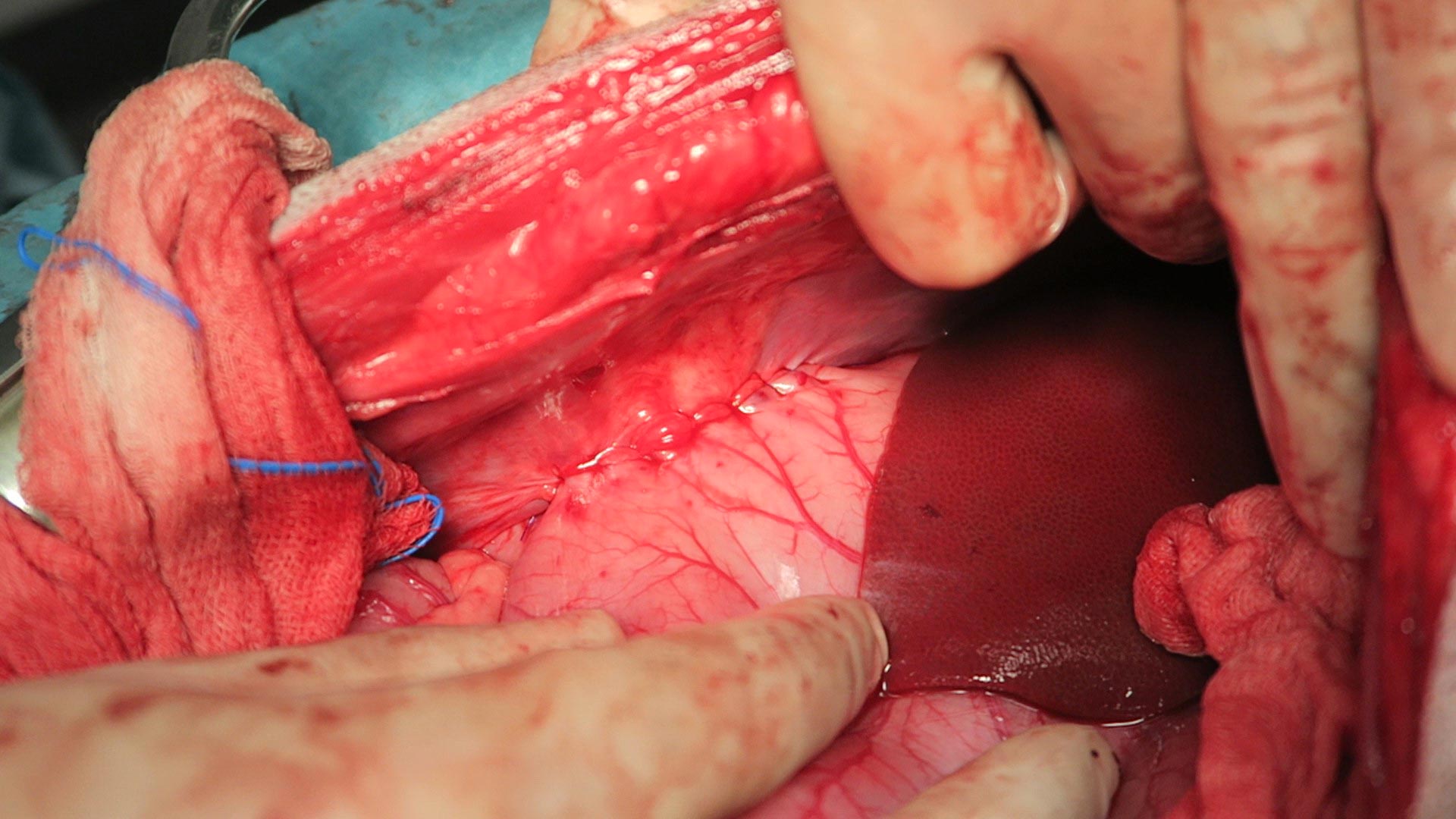
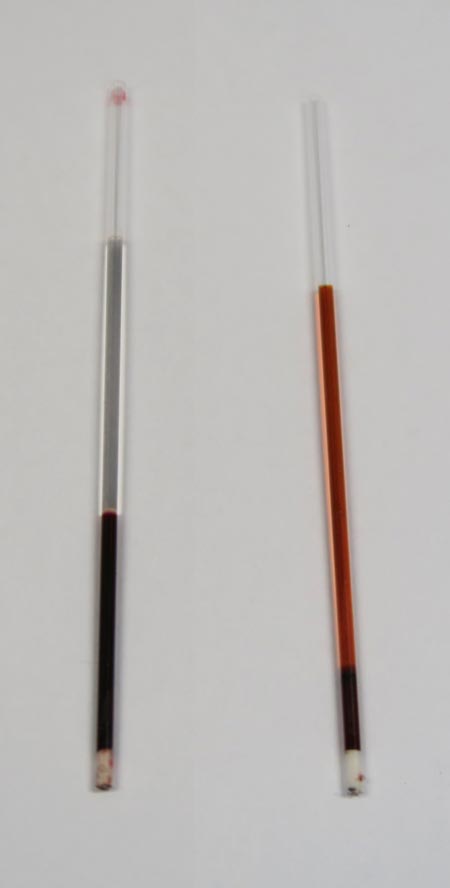
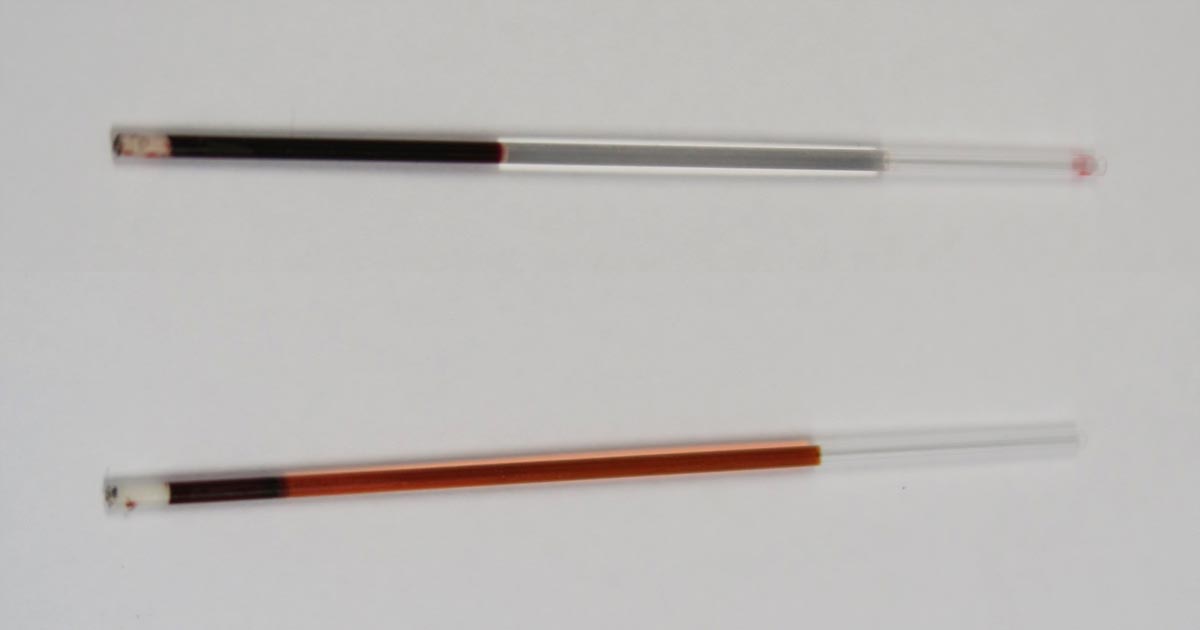
When interpreting the often misinterpreted and underused PCV and total solids test, it is important to take note of the serum colour as this may give clues into the diagnosis.
Normal serum colour (left) compared to a patient with immune-mediated haemolytic anaemia. The serum is haemolysed and anaemia is present.
The most common abnormalities seen in clinic are icteric, haemolysed and lipaemic serum.
Clear serum can also be of importance – especially when you interpret it with blood counts and urine colour.
Haemolysis
The most common abnormality of serum colour changes is haemolysis. In my experience, the most common cause is suboptimal collection technique. To confirm this, simply collect another sample and repeat.
If it is repeatable, and concurrent anaemia or pigmenturia is present, it warrants further investigation.
Intravascular haemolysis can be caused by:
immune-mediated haemolytic anaemia
blood transfusion reactions
infectious diseases such as Mycoplasma haemofelis, Babesia canis, Ehrlichia canis, FeLV and others
Heinz bodies from the ingestion of heavy metal, onions or paracetamol
hypophosphataemia
macroangiopathic disease (neoplasia, for example)
envenomation – typically, snake bites
Testing issues
Haemolysis can also affect other laboratory testing. It can lead to an artefactual increase in glucose, phosphorus, bilirubin, total protein, fructosamine and triglycerides, and a decrease in sodium (pseudohyponatraemia), cholesterol, calcium, potassium and albumin.
Extravascular haemolysis often does not cause haemolysed serum as it is generally slower and the body is able to clear the haemoglobin before it can lead to discolouration of the serum.
Despite that all COVID-19 restrictions are due to be removed as early as the end of the month, the long-term impacts of this pandemic have yet to ease and will likely be sending ripples through many professions for the foreseeable future.
The virus has already left lasting changes to the landscape of the veterinary industry – not only in how it operates, but in how new professionals are taught from the ground up. Long gone are the days of packed-out waiting rooms and lecture theatres.
The more things change
Even with restrictions out of the way, it’s thought that measures put in place over the past two years to reduce viral transmission in our practices may remain the “new normal”, with clients asked to wait outside until necessary, and often with only a single owner asked to come in with their pet at any one time.
Several vet schools now operate under the banner of “blended learning”, whereby the curriculum is taught in a mixture of face-to-face content, live and online lectures, alongside pre-recorded, virtually accessible resources.
In the face of recurrent industrial action – coupled with the rising, desperate demand for new veterinary professionals – online teaching may offer a convenient, long-term solution.
Fallen behind
As with all change, there are pros and cons, although one area I think is yet to be fully addressed is the issue of EMS backlogs.
There are current backlogs in the NHS, the postal system and in many other major industries throughout the country, and I don’t believe the veterinary student training system has escaped unaffected.
For a good 12 to 18 months, many practices – especially small independents – were forced to shut their doors to both pre-clinical and clinical placements – and although EMS requirements were lowered for all year groups due to graduate by 2023, every succeeding year must complete the formerly required 26 weeks.
This has led to an overwhelmingly large number of students competing for a progressively smaller number of placement opportunities.
This makes it particularly difficult for students who lack their own transport, or the funds to travel far from their university or hometown, meaning there may be growing social inequity in the variety and quality of experience vet students are able to obtain.
Better the devil you know
Not only this, but large veterinary conglomerates may have the infrastructure to accommodate larger numbers of students, and new graduates may want to “stick with what they know” and, therefore, be less likely to consider signing contracts with smaller, independent practices.
There is also the argument that, with the rise of online teaching and decrease in student-lecturer contact, work experience has never been such a valuable tool in supplementing a student’s learning.
With the demand for placements higher than ever before, and veterinary practices sometimes two or three times busier than before the pandemic, the financial cost of EMS for some students has never been greater.
Essential experiences
Confidence, satisfaction and a balanced education behind all new graduates serves the interest of both individual professionals, and the profession as a whole.
In my opinion, there has never been a greater need for a review of the need for higher education funding for veterinary students, to allow every student access to a large variety of work experience and the opportunity to see what different avenues are available to them after graduation.
The PCV and total solids (TS) test is simple, yet informative – but is often misinterpreted or underused.
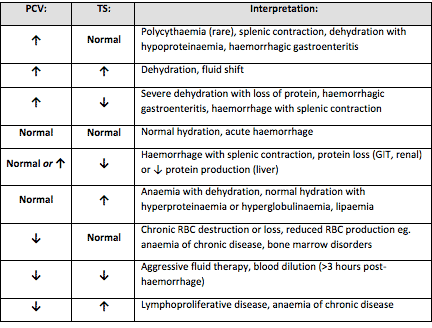
Table 1. Changes that can be found on a PCV/TS and possible causes (click to zoom).
It is important to remember all test results need to be interpreted in light of the patient’s history, presenting clinical signs and general physical examination findings.
The various changes that can be found on a PCV/TS, and the possible causes, are detailed in Table 1. Many of the differentials can be included or excluded based on the history, clinical signs and examination findings.
Misconceptions
I would like to highlight some common misconceptions I find with PCV/TS interpretation.
A normal PCV/TS means the patient cannot be dehydrated
The concept all dehydrated patients will have an elevated PCV/TS is inaccurate. Patients will have to be severely dehydrated to see an elevation in both PCV/TS.
Dehydration should be based primarily on physical examination findings, not based primarily on PCV/TS results.
A patient with a normal PCV could not have lost blood as the PCV should be low
Patients can have acute whole blood loss, which is not reflected in the PCV at presentation. This could have been caused by a number of reasons – for example:
the extravascular fluid has not yet shifted down the hydrostatic pressure gradients
the patient has not ingested water since the time of blood loss
IV fluid has not been given to correct the hypovolaemia
Once the fluid shifts, the patient drinks water or IV fluids are administered, the PCV/TS will drop due to haemodilution.
An elevated PCV means the patient is dehydrated
PCV tubes.
This is probably the most common change I see in my patients – and it is not because they are all dehydrated.
The most common cause of this change is stress-induced splenic contraction. The spleen stores red blood cells. Under the influence of adrenalin, the smooth muscle in the spleen contracts and the stored red blood cells are pushed into circulation.
The next most common cause would be haemorrhagic gastroenteritis, where a fluid shift into the gastrointestinal tract has occurred.
Assessment of the serum colour can also provide valuable information. White or lipaemic serum can cause artifactually high TS. Haemolysed serum with a low PCV can indicate a haemolytic anaemia.
Next time you perform a PCV/TS, look at Table 1 and consider the other differentials for your results.
Last month we discussed the importance of caring for clients during the process of euthanising their much-loved pet. This month, we focus on your patient.
The goals of euthanasia are always to make it as painless, fearless and stress-free as possible for the patient.
Pain relief
Most patients presented for euthanasia are either suffering from chronic, terminal or traumatic disease.
The first thing I like to do is ensure the patient’s pain is managed. This usually means providing opioid pain relief. Methadone is my opioid of choice. Butorphanol provides minimal pain relief, but is excellent for mild sedation.
Next, if your patient is in shock, you need to try to alleviate some of it through IV fluid resuscitation. This is important as poor circulation will slow the process when you administer the euthanasia solution.
Calm and stress-free
One of the most important goals in the euthanasia process is to have the patient as calm and stress-free as possible.
If the patient is stressed or anxious, some sedation may be required. Diazepam or acepromazine are good choices, depending on the condition of the patient, of course, and, together with the opioid you have administered already for pain relief, will help calm the patient. Try to avoid using medetomidine as a sedative in all but the most fractious of patients, as it causes peripheral vasoconstriction that will make IV catheter placement difficult.
The aim of sedation is to relax your patient as much as possible without rendering them unresponsive to owners when it is time to say goodbye. This can be tricky as every patient responds differently to sedation, so you must make a point of warning owners the sedation may make their pets very sleepy.
IV catheter
Where possible, I avoid performing euthanasia without first placing an IV catheter. It makes the delivery of the euthanasia so much smoother. Including an extension to the administration line also allows you to stand a little away from the patient and their owners to give them a little privacy while you administer the euthanasia solution.
Once your patient is sedated and an IV catheter placed, I set up comfortable bedding in the room where I will perform the euthanasia and bring the patient to the room. The amount of euthanasia solution I have with me always exceeds how much I think I will need; the last thing I want is to have to leave the owner and patient to get more euthanasia solution.
Once I have administered the euthanasia solution, I check the heart and once that stops completely, I then tell the owners their pet’s heart has stopped, which they understand as their pet has passed.
Performing euthanasias is the one of the hardest parts of our job, but also a privilege we hold as vets, so I hope my tips will help make the process easier for you, your client and, most importantly, your patient.
Many facets of mental health are comparable to physical illness/fitness, and I’ve gained a lot of introspection on how to keep myself mentally healthy and happy on the vet course from lessons I’ve learned from my physical training.
Since joining the gym a couple months before the pandemic hit (as futile as that turned out to be) to focus on my physical health, I’ve noticed a profound increase in my mental health and my general mood.
There’s a lot that links mental and physical health that we’re barely scratching the surface of. Endorphins released while exercising improve your mood and reduce anxiety, wearing out your body a little more during the day helps you sleep better at night, and building a routine can certainly be beneficial in a course as time-management crucial as veterinary medicine.
Getting physical
Having said that, I think there’s a lot more to it when it comes to prophylactic mental health.
When I started weightlifting, for example, it was easy to feel like more was better – to the point where I was putting in more time in the gym, but seeing less results.
As counterintuitive as this sounds, your body needs time to rest and recover before starting back fresh with renewed levels of energy. Usain Bolt isn’t trying to break records every single day, and being at 110% all the time sounds exhausting… and is probably also impossible.
The same can be said for working and revising. If you have an inbound deadline or exam, your impulse is likely to think that the more you work, the better your grade. But trust me, that’s just not always the case – and I learned this the hard way.
Heed the warning signs
After suffering from burnout in my first year – after three months straight of revision (which I began four months before exams) – I had to accept that, long term, high intensity just isn’t sustainable.
Recently, I’ve been able to apply the warning signs I’ve learned to pick up on at the gym to my work on the vet course.
If I’m noticing that I’m not motivated to work out, that the weight I lifted easily last week now feels super heavy, or my muscles are sore for longer, I know it’s time to tone it down. Similarly, if I can’t bring myself to stare at another textbook, if a fact I previously knew now keeps escaping me, or if I’m noticing longer periods of bad moods and shorter periods of feeling happy, I know that something needs to change.
For the former problem, I take a couple days off, do some stretching, and give myself time to heal. For the latter, the process is much the same, rest, relaxation and doing my best to switch my mind off – whether that’s TV, a good book, or, ironically, a good gym session.
Preventive approach
With the busy work life that comes with being a vet, I think the luxury of being able to go to the gym three or four times a week falls by the wayside, despite even the best of intentions.
I know of a lot of professionals who’ve given up hobbies like running or hiking because there simply aren’t the hours in the day.
However, giving our medical staff the time to take care of their physical health could go a long way to lessening the mental health crisis that has existed in the veterinary community for decades.
Euthanasia is a big part of our work as veterinarians. Working in an emergency setting, it is something I have to face on every shift.
It doesn’t get any easier no matter how many times I have to do it, but I have fine-tuned my approach over the years so each euthanasia process runs as smoothly as possible, with minimal additional stress to both patient and client.
This month, I will talk about taking care of your client.
Communication is key
Euthanasia is a big part of our work as veterinarians.
The most important aspect of taking care of your client in this difficult time is to make sure you really focus on communicating clearly, effectively and, most importantly, with sincere empathy.
First, I listen to their concerns, and why they have made the difficult decision to euthanise their pet.
Quality of life decisions can be a very grey area, and sometimes what you think may be manageable as a veterinarian can be a huge quality of life concern for a pet owner.
A prime example is osteoarthritis in older dogs. You may assess them as being clinically well except for some difficulty walking, but the client sees their pet every day and notices the struggles they go through.
Euthanasia is a difficult conclusion for them to come to and, in most instances, I will defer to the client when it comes to assessing the quality of life of their pet.
Quality assessment
One way I help clients assess their pet’s quality of life is by asking them about a few aspects of it, including:
Can your pet do the things that make them happy?
Do they spend more days sad, depressed and ill compared to the number of days they are bright, happy and eating?
Is your pet in pain? Is this pain manageable?
Confirmation
Once a client has expressed they want to euthanise their pet, I always try to confirm three things:
That they have actually decided to euthanise their pet. I frame the question like: “So, my understanding from our conversation is that you have made the decision to euthanise Fluffy today?” Sometimes, when you ask this question, the client reveals they have not actually come to that decision yet, which means you will need to backtrack a little and guide them through the decision process again.
Whether they would like to be present for the euthanasia.
How they would like us to handle the after care.
I also always try to manage all documentation and finances before the euthanasia so the clients will be in a position to leave immediately after the procedure, meaning they can begin to grieve rather than have to do paperwork. The only exception to this is when the patient is in a critical condition, meaning euthanasia cannot wait.
Explaining the process
Try not to perform the euthanasia in your consult room or in the main treatment areas – if you have a private room for euthanasias, that is the most ideal. This is important especially if the client comes back in the future with another pet or a new pet. They often find it difficult to walk into your consult room and be reminded of the euthanasia of their beloved pet.
I like to give clients some time to spend alone with their pet to say their goodbyes in private. When I come back into the room, I start by explaining the process of the euthanasia, covering the following things every single time:
Euthanasia is an overdose of an anaesthetic agent
The process is quick – 10 to 20 seconds
It is completely painless
The pet doesn’t close their eyes afterwards
The pet can have a couple deep breaths and muscle tremors
The pet can release their bowels and bladder (especially important to warn of this if the clients want to hold their pet)
Lastly, if their pet came into the hospital in shock and obtunded, where I have fluid resuscitated them, meaning they are now more bright and alert, I warn the clients that despite their pet looking better, the underlying disease remains the same.
Once the euthanasia is performed, I again ask if the client wants to spend a little more time in private with their pet. Finally, when the client leaves, they typically will say “thank you”.
Whatever you do, do not say something like “my pleasure” or “you’re welcome” like you would for a vaccination consult – this is a natural response, but would be a terrible faux pas. I simply say “I’m very sorry for your loss. Take care for now and let us know if we can help in any way”.
Next month, I will talk about taking care of your patient throughout the euthanasia process.
This month, we will look at the final part of a fluid therapy plan – accounting for ongoing losses. This can be challenging, but some general rules can be helpful.
Regular assessment is essential to track patients’ responses.
When considering ongoing losses, try to not forget about patients with pre-existing polyuric diseases; chronic renal failure is a prime example. Patients with dehydrated chronic renal failure are unlikely to suddenly regain concentrating ability. Polyuria should be considered as an ongoing loss.
Other conditions that may result in additional urinary fluid losses include post-obstructive diuresis, diabetes mellitus, hyperadrenocorticism and hyperthyroidsim.
How much to add?
This is the tricky part. I often add an additional half to one maintenance and frequently reassess clinical parameters, or if a urinary catheter is placed matching ins and outs.
Gastrointestinal tract losses can be collected and weighed; 1g of vomitus or diarrhoea can be roughly equivalent to 1ml of water.
Fluid removed from drains placed in cavities or wounds should also be measured and accounted for.
Remember the key point is regular assessment of the patient’s hydration status, from repeat clinical exams, to track their response. Don’t forget regular retesting of electrolytes – for example, every 12 to 24 hours for patients on IV fluids and not eating.
Vets have to handle a variety of difficult situations, from delivering bad news to addressing financial difficulties. But when it comes to tackling client grief, awkwardness or anger, it’s a bit like that old children’s book, We’re Going on a Bear Hunt – we can’t go over, under or around it – we’ve got to go through it!
I recently had a three-hour communications practical, during which my fellow students and I were tossed into a randomly selected clinical scenario designed to help us deal with uncomfortable areas of future practice. These included such topics as:
discussing the needs for euthanasia
apologising for clinical mistakes
reasoning with angry farmers when their herds came back TB-positive
Role play
We’re Going on a Bear Hunt, written by Michael Rosen and illustrated by Helen Oxenbury, is available from Amazon.co.uk and other booksellers.
All scenarios were conducted with real actors portraying the clients – and although we’d been given a list of topics to revise if we wanted – any revision turned out to be next to useless as the exercise was less about what you knew, and more about how you dealt with people.
Personally, I find this type of practical as rewarding – if not more so – than our clinical skills work. We have countless opportunities to practise suturing, spaying and catheterising in the labs at school, and in final-year rotations, but dealing with the raw side of client communications is the one thing we never actually get to experience until we’re suddenly in the driver’s seat.
It’s completely understandable – nobody wants a student present at their most vulnerable moments. If my own pet was being put down, I’d want the comfort of an experienced vet doing the job and walking me through it from start to finish.
Learning experiences
That’s why I think communication practicals are so incredibly useful, and it’s a real shame that I’ve only had three in my course so far. It can be difficult to learn from and build upon experiences spaced years apart from one another, and I feel incredibly sorry for the year before me (while I was intercalating) who had to do their scenarios over Zoom.
One of the most valuable lessons that these practicals have taught me, is not to be afraid of emotion.
It can be difficult – especially when a very valid defence mechanism for many medical professionals is to distance yourself from it at all costs – but there are moments when all is required of you is simply to be there, to listen and understand.
Just be there
There’s no textbook in the world that can teach you that. When a client (or an actor pretending to be a client) is crying in front of you, you want to fix their grief because fixing things is, quite literally, your profession.
Your instinct is to talk and fill the silence, but instead, you need to wait for them to process the moment and then be there to answer their questions.
Some things you can’t fix and you can’t work around – you just have to go through them.
Postoperatively, gastric dilatation-volvulus (GDV) patients remain in our intensive care unit for at least two to three days.
Monitoring includes standard general physical examination parameters, invasive arterial blood pressures, ECG, urine output via urinary catheter and pain scoring.
I repeat PCV/total protein, lactate, blood gas and activated clotting times (ACT) immediately postoperatively and then every 8-12 hours, depending on abnormalities and patient progress.
Patient recovering in the pet intensive care unit. As well as standard monitoring parameters, GDV patients have constant ECG, arterial blood pressure and urine output monitoring to enable the early detection and correction of abnormalities.
I always repeat these blood tests postoperatively, as IV fluids given during the resuscitation and intraoperative period often cause derangements. I use the results to guide my fluid therapy, but also take it with a grain of salt.
IV fluids
I generally continue a balanced and buffered crystalloid. The rate depends on blood pressures, urine output and assessment of general physical examination parameters for perfusion and hydration, but I try to avoid fluid overload and reduce the IV fluids postoperatively as soon as possible.
Coagulopathy
Prolonged clotting times are frequently seen as a result of consumption in a dog with GDV. However, one should note it can also occur as the result of haemodilution.
As the underlying disease process has been corrected, and haemostasis achieved during surgery, I usually monitor ACTs, but may not necessarily treat with blood products as prolonged ACTs do not always translate to clinical bleeding. Unless clinical evidence of bleeding exists, I generally hold off treatment and monitor.
Hypoproteinaemia
Low total protein is also common. This is generally due to haemodilution from fluid resuscitation. However, a low total protein does not mean oedema will develop, or that it requires management. I generally track the protein levels, use conservative fluid therapy and try to correct it by instituting enteral nutrition as soon as possible.
Electrolyte imbalances
Hypokalaemia is a common complication of fluid therapy. This can be rectified with potassium supplementation in the IV fluids.
Hyperlactataemia
If present post-surgery, this is usually corrected with a fluid bolus. However, I always assess for other things that may affect oxygen delivery to the tissues, such as poor cardiac output (arrthymias), hypoxaemia (respiratory disease) and anaemia (from surgical blood loss).
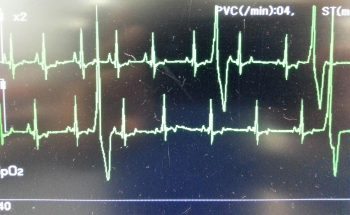
Arrhythmias
Ventricular arrhythmias are common post-surgery. Accelerated idioventricular rhythms are the most common cause, especially if a splenectomy was performed.
Ventricular premature contractions are common postoperative arrhythmia.
Before reaching for anti-arrythmia medications, first check and correct:
electrolyte abnormalities
hypoxaemia
pain control
hypovolaemia or hypotension
If they are still present, despite correction of the above, consider treating the rhythm if:
multifocal beats (ventricular premature contractions of various sizes)
overall rate greater than 190 beats per minute
R-on-T phenomenon
low blood pressure during a run of ventricular premature contractions
I start with a bolus 2mg/kg lidocaine IV and start a constant-rate infusion of 50ug/kg/min to 75ug/kg/min.
Anaemia
It is common to have a mild anaemia post-surgery, due to a combination of blood loss and haemodilution. In the absence of transfusion triggers – such as increased heart rate, increased respiratory rate or hyperlactataemia – it does not require treatment.
Vomiting
Anti-emetics are the first line of medication. Non-prokinetic anti-emetics, such as maropitant and ondansetron, can be used immediately; otherwise, after 12 hours, metoclopramide can also be used postoperatively. If the patient remains nauseous despite these medications, the placement of a nasogastric tube can ease nausea by removing static gastric fluid.
Excessive pain relief may also contribute to the nauseous state.
Pain relief
I mostly rely on potent-pure opioid agonists, such as fentanyl constant-rate infusions and patches. This is generally sufficient for most patients. Ketamine is occasionally used.
Some drugs listed in this article are used under the cascade.
Following on closely from the first two parts of our February focus on gastric dilatation-volvulus (GDV) – which covered IV fluid resuscitation, pain relief and gastric decompression – we turn to surgery.
Here, I offer a few tips to help ensure the procedure runs as smoothly as possible.
Abdominal incision
Make the abdominal incision large – from the xipoid to the pubis. You cannot perform a proper exploratory laparotomy without proper visualisation. Additionally, when it comes time to re-rotate the spleen, you will need all the space you can get. Removal the falciform fat to help improve exposure.
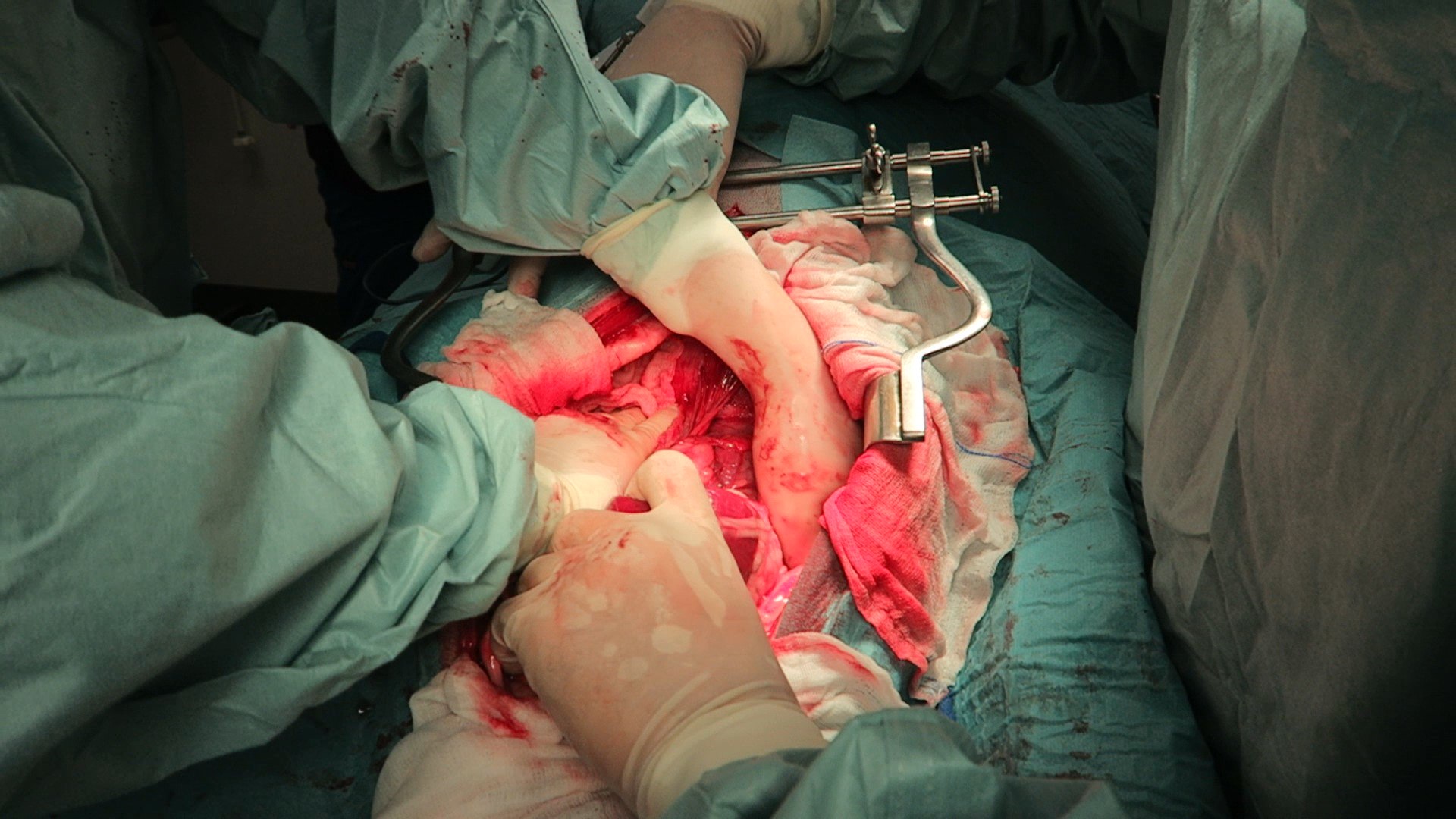
Derotation
Figure 1. Derotation of the stomach. Standing on the right side of the patient, one hand pulls as the other pushes.
The degree of rotation is variable from 90° to 360°, so not all GDV surgeries will be the same. If the omentum is draped over the stomach, this is pathognomonic for GDV.
When derotating, stand on the right side of the patient as all descriptions are based with the surgeon on that side.
During volvulus, the pylorus rotates ventrally then to across to the left side of the body.
Method
With one hand (usually your right) reach down the left abdominal wall and firmly grab the stomach down where the spleen normally resides, then pull towards you (Figure 1). At the same time, use your other hand to apply downward pressure (or pressure in the dorsal direction) on the right side of the stomach. This simultaneous pulling on the left side of the stomach and push on the right side of the stomach is generally successful.
At this stage, it is important to check things have gone back to their normal places. Ensure the:
pylorus is to the right and you are able to track it through to the duodenum and pancreas
fundus is to the left
omentum is hanging off the caudal aspect of the stomach
spleen is also derotated
Passing a stomach tube can sometimes help you identify the oesophagus – you can feel it running along the inside of the gastric cardia and fundus.
Further decompression
If the stomach is still distended and hard to manipulate, reducing the size of the stomach can make derotation significantly easier. Pass the stomach tube again or aspirate more gas from the stomach using a 18G needle, extension set, 50ml syringe and three-way tap.
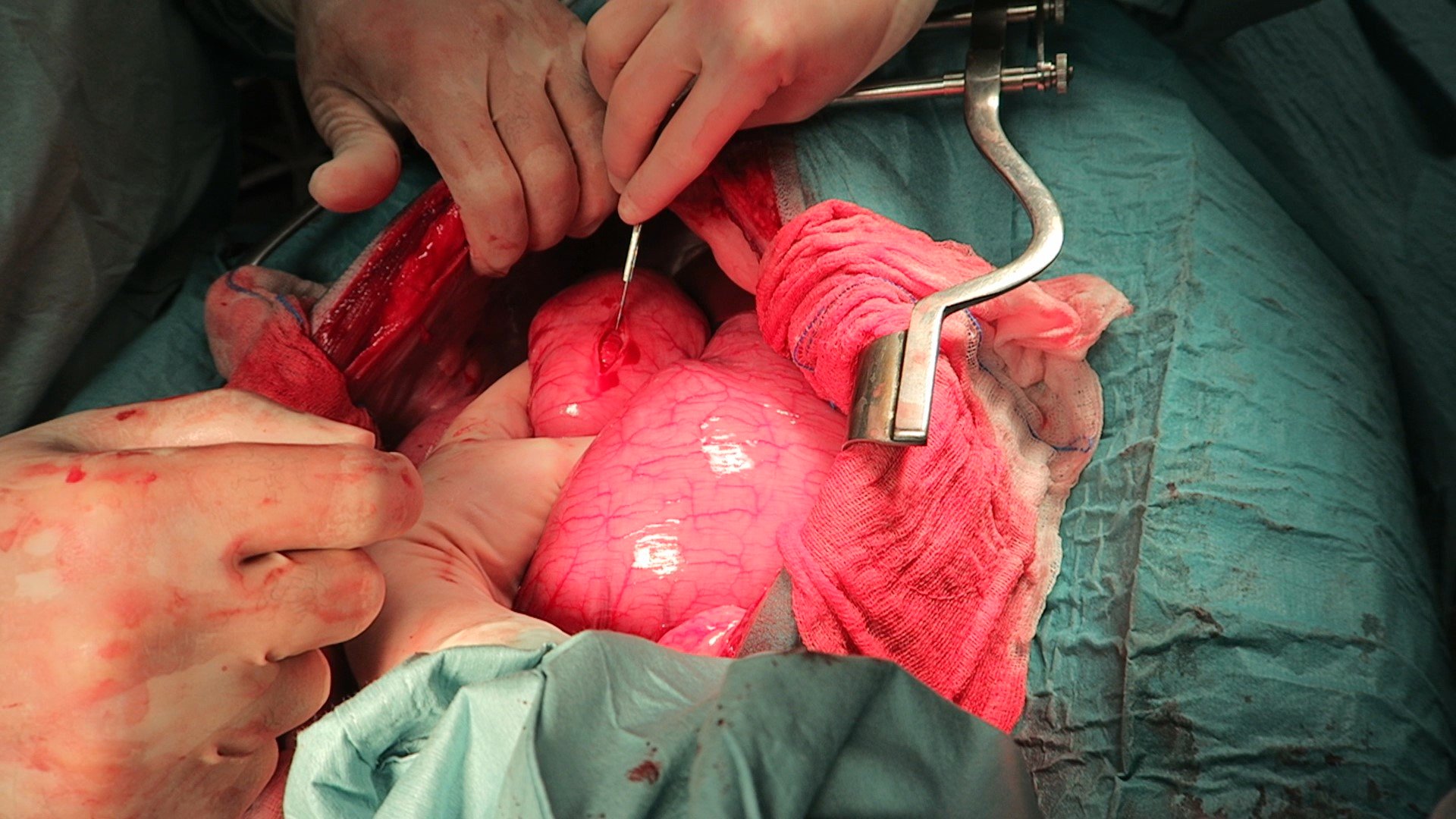
Assessment of the stomach
Figure 2. Incision into the pyloric region of the stomach.
Figure 3. Completed incisional gastropexy.
Gastric necrosis is most likely to occur along the greater curvature of the body and fundus. Lifting up the stomach and looking at the dorsal aspect of these areas is important. Allow 5 to 10 minutes after derotation before resecting the affected areas to see if it regains colour and pulsations.
Pexy
I personally perform incisional gastropexy – I find them easier and very effective. I find an area on the pyloric region of the stomach where minimal tension exists, when brought to the lateral body wall (Figures 2 and 3).
Ensure you do not accidentally incise into the diaphragm; the muscle fibres of the diaphragm radiate out and insert at the costal arch. Identify the transverse abdominal muscles and pexy the stomach to here.
I also ensure muscularis to abdominal muscle contact to increase the strength of the pexy once it is healed.
Spleen
The spleen is almost always engorged in GDV cases, but this does not necessarily mean it needs to be removed.
Always assess the splenic blood supply as it is not uncommon for splenic vessels to tear or thrombose during the volvulus.
If there is any concern that the splenic arterial flow is compromised, I would perform a splenectomy.
Stomach still dilated after pexy?
What if the stomach appears to be still dilated? Generally, once the stomach is derotated, normal anatomy has been achieved and the pexy is performed, the remaining food and gas will pass with time. You can try to empty more via a stomach tube or aspiration with a large needle, but this is not generally required. I would not perform a gastrotomy to remove contents.
Next week, we will cover common postoperative complications.








 The process is quick – 10 to 20 seconds
The process is quick – 10 to 20 seconds