Acid-base disturbances are common in critical patients. These changes must be identified, as even minor deviations from the normal range can lead to significant abnormal body functions.
Acidaemia and alkalaemia
Acidaemia, which occurs when blood pH falls below 7.35, will lead to:
impedance of cardiac output
reduced cardiac contractility
a blunted response to catecholamine manifesting as hypotension
antagonism to insulin
a compensatory hyperkalaemia (extracellular movement of potassium in exchange for hydrogen ions [H+])
Alkalaemia – blood pH above 7.45 – although less critical compared to acidosis, will result in:
muscle spasm
stuporous mentation
hypocalcaemia
hypokalaemia (intracellular movement of potassium in exchange for H+)
As well as the aforementioned altered functions, H+ is essential for the normal function of enzymes and maintenance of normal cell structures. This is why the body maintains a very narrow pH range and uses multiple buffering mechanisms to achieve this.
Buffering systems
The two main buffering systems are the kidneys and lungs.
Kidneys adjust the pH via the excretion of H+ and the uptake of bicarbonate (HCO3-), which is the primary extracellular buffer and has a linear relationship with pH.
An increase in HCO3– concentration will result in a pH increase and vice versa. This mechanism can take hours or days from the time a shift in the pH is detected.
The main respiratory buffer is CO2 – an acid. CO2 has an inverse relationship with pH, so an increase is equivalent to a lower pH level and vice versa. The effect of respiratory adjustments is immediate. This occurs by altering the respiratory rate to adjust CO2 levels.
The first step towards interpretation of acid-base disturbances is identifying whether an alkalaemia or acidaemia is present. The next blog will discuss determining what is causing it – identifying the primary disorder and the compensatory mechanism employed to balance it out.
For those of you who have received referral histories from emergency or specialists hospitals, blood gas analysis is probably no stranger to you. For those who have never heard of them before, fear not – you are in for a treat.
In my emergency hospital, the blood gas analyser is arguably one of the most frequently used bench top lab machines, second only to centrifuge, and for good reasons…
Acid-base disturbances are common in critically ill and emergency patients, and it can help determine the severity of their condition and sometimes provide the answer. Tracking changes in blood gas parameters can provide information about the patient’s response to your interventions.
Blood gas analysis can help assess the severity of a patient’s condition and help guide your diagnostic plan.
The information gained from pulse oximetry is very limited in patients with severe respiratory compromise, and the only way to accurately assess their oxygenation and/or ventilation status is by looking at their blood gas status.
So what does the blood gas analysis actually measure?
Most blood gas panels assess the pH of the blood, partial pressure of oxygen (PO2) and partial pressure of carbon dioxide (PCO2). From these, the machine is able to derive the percentage of haemoglobin saturated with oxygen (SO2), bicarbonate (HCO3–) concentration and base excess of the extracellular fluid (BEecf).
In most machines, they are also able to measure other parameters, such as electrolytes (Na, K, Ca, Cl), glucose and lactate.
While arterial blood gas samples are required for determining the ability of the body to oxygenate the haemoglobin, venous samples are suitable for determining the ventilation status, assessing acid base balance, electrolytes, glucose and lactate levels.
So how can this help as a point-of-care test?
As mentioned previously, blood gas analysis can help assess the severity of a patient’s condition and help guide your diagnostic plan. It can also provide a diagnosis (such as diabetic ketoacidosis, typical hypoadrenocorticism and high gastrointestinal obstructions).
The changes in these parameters over time can be essential in managing critical patients in the emergency setting; it will help guide you in developing an appropriate IV fluid therapy regime and fluid choice, address the patient’s oxygenation and/or ventilation needs, correct any electrolyte and glucose abnormalities, and – although fallen out of favour – the administration of sodium-bicarbonate therapy.
In upcoming blogs, I will teach you how to interpret the blood gas results. At the end of this, I hope everyone will incorporate blood gas analysis as their standard point-of-care test for the better assessment and management of patients.
If given the choice between a biochemistry and a blood gas panel in a critical patient, I would hands down select blood gas every time.
The cost of living has risen sharply in the past year. Food, bills, and fuel costs seem suddenly extortionate and yet student loans haven’t budged an inch – meaning students are paying more for food, bills and other essentials than ever before, with relatively less financial aid.
Vet students in particular are no strangers to stretching the pound – we’re in it for the long haul after all, so five to six years of rent, utilities and food, with little to no income is something most of us have to accept as par for the course.
The tricky thing is that while food bills can be lowered by steering free of Deliveroo and “Taste the Difference”, and opting for the simpler things in life, and a couple of extra jumpers helps lower heating costs in the winter, there’s really no way of getting around the current fuel crisis.
You’ll go far
The reality of EMS in the current climate is that many students are still trying to replace pre-clinical and clinical placements that were cancelled during the pandemic, and a lot of veterinary conglomerates have contractual obligations to a specific university.
With the number of vet schools on the rise, “freelance” placements are going to become thinner on the ground, and if (like me) you live close to one of these vet schools, you may need to travel farther afield for your EMS placements.
This means not only has the cost of living increased for students in general, but the cost of education for veterinary students is also on the up.
Automotive breakdown
For the average engine, the cost of a mile’s journey in June was 16p (according to the RAC Fuel and Mileage calculator), whereas placements can range from within walking distance to over an hour’s drive away. If a student has a daily commute of just 13 miles (roughly a 15 to 20 minute drive) each way, for two weeks – even if they let their car run right down to the red – they’d still be spending more than £40 on fuel.
For longer commutes, or ones where vets expect students to follow in their own cars on callouts, it’s easy to see how the costs can get out of control.
Covering costs
Veterinary students are required to fulfil a minimum 26 weeks of work experience during their clinical years. For those unable to find placements near their university or home accommodation, or unable to find affordable accommodation near the placement itself, commuting is a necessity to gain the experience and accreditation needed for their degree.
For a long time the veterinary industry has been striving to improve its inclusivity and accessibility, but with fuel prices hitting an all-time high this year, travel bursaries may be a real necessity in ensuring the degree is not made unaffordable.
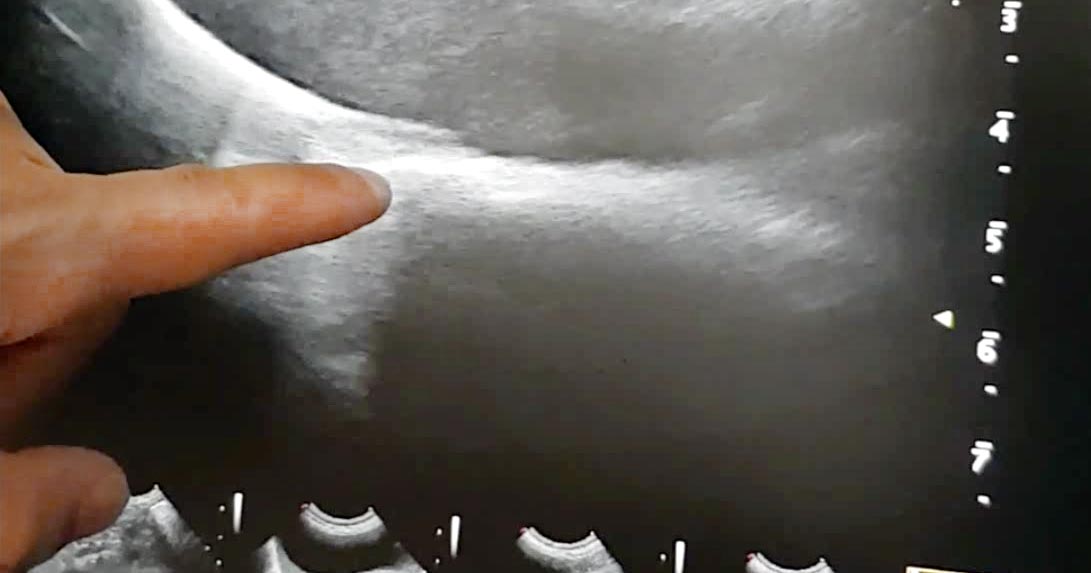
Assessment of the caudal vena cava, via the diaphragmatic hepatic view, is useful for assessing the volume status of a patient.
This is particularly helpful for hypotensive patients, to check whether they require more volume or vasopressor agents, or other management. With regards to “more volume”, this could be crystalloids, colloids or blood products, depending on the patient.
How to find it
Place the probe under the xiphoid process.
Increase the depth, adjust the focal point, then reduce the frequency to be able to visualise the diaphragm completely.
Find the gall bladder, fan laterally to the right (slightly).
The caudal vena cava is seen deep to the gall bladder as two parallel lines through the diaphragm wall.
Assessment of volume status – or, more so, fluid responsiveness – is based on interpretation of the degree of collapse during inspiration.
Interpretation
If it does not collapse during inspiration (“fat”), this can mean the vena cava is adequately loaded or volume overloaded. These patients would most likely benefit from vasopressor agents (or other managements – for example, pericardiocentesis), rather than further volume.
If it collapses more than 60% (“flat”), the patient requires more volume.
If it collapses between 20% to 60% (“bounce”), further volume loading can be trialled.
If you don’t come from a “horsey background” (like me) then the equine side of the vet course can feel a little overwhelming.
From a different number of ribs and guttural pouches to the inability to vomit, horses have an abundance of clinical differences to our smaller patients, and so (quite rightly) often need to be studied in their own right, much the same as with farm animal medicine.
Clinical aspects aside, the world of equine also comes with a wealth of nomenclature that seemed to me, at first, like a second language. A disease called “glanders and farcy” was a particular favourite equine term of mine, as it sounds deceptively quaint despite in fact being an incredibly serious and often fatal notifiable disease.
For these reasons, in all honesty, I was a little apprehensive of my first equine clinical placement – most likely not helped by a distinct lack of large animal clinical EMS up until that point (thank you COVID-19).
As it turns out however, the two-week placement became one of my favourite so far. So, for those of you with it still to come, here are a few things I wish I’d known going in…
Time to smell the hay
Small animal medicine can sometimes be fast paced, and patients can come and go in a blur. With 15-minute consults and a lot to pack in within that time, there sometimes just aren’t the opportunities for students to ask questions or for advice.
On the other hand, equine and large animal medicine placements are often a little less patient intensive, affording students the opportunity to really dive into each individual case, rather than losing track of how many they’ve already seen that morning.
The drive between clients can also provide time for asking questions, filing in your case logs for the last animal, and reading up on the next.
Communication, communication, communication
Depending on the client, of course, a lot of call outs will involve a certain amount of time standing around the horse with the client waiting patiently at the reigns.
Dentals, in particular, can take a surprisingly long time and while in small animal practice the vet can typically just stick the radio on, plonk on a stool and get to it, that might seem rather rude with the animals owner standing right next to you. Being able to hold a conversation with the client, whether its about their animal or just the nice weather we’ve been having, is a skill that can sometimes be sidelined in favour of clinical competencies.
Making conversation can also be extra difficult if you’re trying to be clinically competent at the same time – and this is where multitasking comes in, as vets will often have to engage with the client for more than an hour while performing tasks on the animal that a smallies vet would probably take a dog out the back to do.
As a student, spending long periods of time with a vet and a single client is a great opportunity to practice client engagement and communication. If in doubt, and you’re left alone with the owner while the vet runs back to their car, try asking about their animal (how long they’ve had it, if it’s their first, and so on). We all love gushing over our pets, and it goes a long way to show enthusiasm instead of the vet coming back only to find the two of you staring in silence at the grass.
When you’re not feeling 100% on your catheter placement or blood sampling, it helps to have something big to aim for. This is where horses come in…
It’s almost like they’ve gone out of their way to be the perfect injection-giving training wheels, with jugulars like drain pipes and large obvious muscle bellies for you to grab in one hand and pop a needle in with the other. Once you’ve mastered the horse IV and IM, it’s only a matter of sizing down.
My main takeaway from this placement was a reminder not to shy away from practising things that don’t come naturally, or aren’t your favourite thing in the world. There’s no point practising the things you know you’re best at, for the sake of feeling good about succeeding in something you already knew how to do.
You’ll feel much better after that initial leap out of your comfort zone, when you succeed in something you couldn’t do before.
I’m only a few short weeks into my final-year rotations at the University of Bristol’s Veterinary Referral Hospital, but I already feel like I’ve learned a lot:
DOPs aren’t as scary as I’d built them up to be in my head.
It does get easier to navigate your way around the hospital with time (and trial and error).
There are quite a few differences between first-opinion and second-opinion practice that I’d never really considered until now.
Budgets
The gift that is the NHS can certainly make us blind to the costs of routine medical procedures. Something as simple as an ultrasound, blood work and a couple of days’ hospitalisation can amass a bill that’s simply unaffordable for a lot of pet owners.
I’ve seen a lot of cases reach the end of the road due to lack of funds, when the answer (or potential answer) was frustratingly simple, but just too much money. The reality of referral practice, however, is that if your patient has made it to you in the first place, there is likely a higher budget to play with than the average consult.
When you’re on a certain rotation, you find yourself doing the same diagnostics every day, so it’s easy to lose track of the value of the drug you’re administering, or the probe in your hand. I think my group and I honestly balked when the cardiology team told us the cost of a standard echocardiogram at the end of our week where we’d been observing between 6 to 10 a day. Of course, it’s still important to keep costs low wherever possible, but it’s been interesting to see how larger budgets and insurance policies are broken down.
Seeing small animal CTs, echocardiograms and neurosurgeries for the first time was an amazing experience, but I do need to keep reminding myself that the proportion of my future patients that will go on to have these sorts of procedures is incredibly small.
When you’re learning in a veterinary hospital, you’re constantly surrounded by leading experts in the field of everything under the sun, and sometimes it’s hard not to feel like a monkey with a stethoscope. Usually, in first opinion, there’s an assortment of different strengths throughout the practice – one vet may have intercalated in neurology and behaviour, while another may has done more CPD on exotic animal medicine. These differences are an asset to every practice and make team working an essential and valuable commodity.
In a referral setting, these “strengths” are often extended to actual specialisms, where the vets are not only actively involved in research in a particular field, but see only animals in a certain category of illness. The need for teamwork, however, is just as paramount here – if not more so!
After working in cardiology for a week and beginning to feel like I didn’t know anything, I can tell you that it was very refreshing to have the head of another department pop their head through the door and ask what on earth was going on with their patient’s heart. When they also didn’t know the actions of all the drugs I’d been painstakingly trying to commit to memory for the past five days, that too came as a wave of relief.
Client communication
Good communication and patience come hand in hand. If you’re delivering bad news to a client or talking them through a complicated diagnosis or treatment plan, that takes time – and although the average first opinion consult is only 15 minutes long, I’d say that, rather oxymoronically, there’s more time to deal with difficult situations in that scenario than in emergency referral.
Of course, first opinion sees it’s share of emergencies as well, but for the most part vets see a disease present slowly over time and are able to prepare their clients accordingly.
In the past couple of weeks, however, I’ve seen referral vets have to delicately balance client communication with the urgency of life-threatening conditions. Sometimes there are mere minutes to intervene after an animal enters the hospital, and vets must be very diligent and considerate when explaining this situation to an owner who may not yet grasp the severity. Owners have to have informed consent at all times, and to be prepared and supported in the event of any potential outcomes, but the sooner an animal is triaged and either treated or prepped for surgery the better.
I think that this is where the truly brilliant vets really shine. To have compassion and humanity at the forefront, with animal welfare and haste also in mind, takes a lot of mental and emotional gymnastics. I’m honestly in awe of every vet I’ve seen both in the past few weeks and over my years seeing practice who’s had to deal with a crisis on both the animal and the human end.
As of yet, I’m unsure if my career will lead me to first opinion or referral practice, but I can appreciate the similarities and differences between the two – despite us all starting out in the same place.
When the unexpected occurs and patients come through our emergency clinic doors, we will often face times when owners become very difficult to deal with. Understanding where they are coming from may help diffuse the situation, but not unless you have good communication skills.
It’s very a very natural response to become defensive when someone acts aggressively and when you feel threatened, but unfortunately this reaction is counterproductive.
You want to be able to treat their pet and help them, but instead your focus can shift to needing to defend yourself and calm them down.
However, the last thing you want to do is advise your client to “calm down”.
Understand the client
Being able to recognise the five stages of grief can help us understand and deal with the situation more effectively. These are:
denial
anger
bargaining
depression
acceptance
Unfortunately, more often than not, it’s nurses and receptionists on the front line who often bear the brunt of this, and it is our job as vets to help them through this process. We need to remind ourselves not to take things personally, as these owners are upset only at the situation and circumstances, not at us.
We need to remain calm at all times and reassure the owners we are here to help them. Owners’ frustration often stems from helplessness and guilt – we all know situations involving much-loved pets can often be driven by anxiety and are highly emotive.
Other times it is because they feel their concerns have not been heard. If you suspect this, you can ask them specifically what they want from us and you’d be surprised how quickly the situation can be resolved once an understanding is reached.
Listen to the client
The Kübler-Ross model, or the five stages of grief, postulates a series of emotions experienced by those experiencing any form of personal loss. IMAGE: raywoo / Fotolia.
It is important to listen without judgement or interruption – although we all know that’s easier said than done.
Showing genuine empathy and acknowledging clients’ emotions and concerns can help you quickly build trust with owners. Even if you don’t know all the answers, let them know you are there for the same reason – you both want to help their pet.
As some of you may have experienced, the most emotional owners can often turn out to be some of a vet’s best clients.
Saying that, if you ever feel you are in danger, or that you are unsure of how to handle a situation, always consult with a more experienced colleague or speak with the vet in charge of the case.
It may be advisable to have a practised line of communication, which shows compassion and understanding but removes you from the situation, where you can get additional support or help.
I see every day our veterinary nurses wear their hearts on their sleeves, and difficult clients can sometimes really hurt them. With this in mind, it is important a nurse can have some breathing time and regroup ready for the next client.
We know nurses want nothing more than the best for the pets in their care. Each case will be different, each client will respond differently, so, like we say in emergency, you have to expect the unexpected.
One thing we do know – your veterinarian will never question a nurse’s compassion. When it comes to client communication and pet care, we will always be a team looking out for one another.
Before coming to university, I never really gave much thought to the life or journey of my food before it ended up on my plate; I wasn’t well informed on the topics of air miles, methane production or abattoir welfare standards.
If you had asked me if I wanted to make sure the foods I ate were ethically sourced, had a low carbon footprint, or had once lived a healthy and happy life, I would have said “of course” – all of these things mattered to me on a subliminal level, but I don’t think I really grasped how any of these concepts were within my control.
Welfare
Animal welfare makes up such a large part of the veterinary course from the very first year, so it’s no wonder so many students are vegetarian or vegan by the time they graduate. I must admit that my Easter Sunday lunch was a little hard to swallow after my first-year lambing placement… and one week on a pig farm certainly had me seeing my Christmas pigs in blankets in a whole new light.
The vet course provides a window into the side of meat production the public will never access – and may not even want to.
In an ideal world (where every animal has a full and healthy life devoid of stress, discomfort or suffering before it is killed), I would have no qualms about eating meat, but the sad truth is that’s just economically and logistically unviable – at least for now.
But welfare isn’t as cut and dried as people might think. Take cows, for example: if you picture a happy cow, it’s probably roaming around in a field, right? Well, frustratingly, fields have many disadvantages – offering parasites, botulism and rogue pieces of metal, while providing no protection from the elements, nor a means for the farmer to moderate their food intake to ward off laminitis, hypocalcaemia and a bunch of other welfare issues.
Along with owning a pair of flared jeans, or developing calves of steel thanks to the endless hills, you didn’t go to the University of Bristol unless you’ve developed a complex over your carbon footprint.
One of the simplest ways to be more environmentally friendly is to eat less meat, but many studies are showing that a global move to veganism/vegetarianism is not the answer for our ever-growing population. A lot of land just isn’t suitable for crops, and rice farming already makes up more than 10% of global methane production.
Again, if we were looking for an ideal scenario, it would be to eat less meat, sourced locally and sustainably, and to value it enough to pay a price that would allow farmers to invest in greener technologies.
Student budgets
Working on farms at all levels of the course gives vet students an appreciation for how much farmers care about their animals, and how hard they work to balance that priority with sustaining a business. Even if you’re sceptical about the meat industry, there is always the option to do research into the farms and butchers that are close to you.
Frustratingly, making good choices from both a welfare and environmental perspective can be much pricier than the alternatives, and this has been one of my own drivers for decreasing my meat consumption during my uni career. Despite this, I still try very hard to make informed choices, and when I do buy meat I aim to prioritise quality over quantity wherever possible.
In very small, but meaningful ways, change is shaped by the decisions and purchases we all make, and understanding the steps that brought the ingredients from the farm to your plate fosters a respect and appreciation for what you are eating, beyond just its taste.
While we know nurses join the veterinary profession for their love of animals, there is so much more to their job description. Veterinary nurses wear many hats covering so many important roles within the clinic.
As with veterinarians, client communication is a vital component of their job and can often be one of the most challenging.
Conveying compassion
Client communication is a vital component of a veterinary nurse’s job.
One thing I have learned to appreciate about nurses is their endless supply of compassion for their patients. Having the ability to convey this compassion to an owner is a sure-fire way to develop a positive relationship, which is the veterinary dream.
Admitting a beloved pet to hospital can be a stressful time for owners. They don’t understand what happens behind the scenes, they just know their pride-and-joy is disappearing into the unknown with someone they have likely never met.
Owners have a tendency to ask nurses questions they were either too shy to ask the vet, or too overwhelmed to remember to ask during their consultation, so I decided to ask the nurses at Animal Emergency Service how they reassure our clients during the admission process.
Offering reassurance
Here are some tips our nurses find useful when dealing with clients:
Introduce yourself and let them know their pet is in exceptional hands.
Know the pet’s name and why it is at the hospital.
Understand the procedures their pet is undergoing while in your care.
Let them know they are welcome to call and you will be happy to inform them how their pet is getting on while in hospital.
Never tell them everything will be fine. You can never be sure with medical procedures, but reassure them they are in the best hands possible – their pet is being treated as if it was your own pet in hospital.
Make them feel their pet is special. Most clients are under the impression their pet is the only patient in the hospital and is essentially the most important pet you’re dealing with that day.
Let owners know their furry friend is comfortable and relaxed in hospital, and receiving an abundance of love. Happy patients make for happy clients and if anyone can reassure an owner his or her pet is receiving the love it deserves, it’s a warm-hearted nurse – just another reason nurses are known as the hearts of our clinics.
Veterinary nurses – the doting advocates and voices for the pets in our practices and hospitals.
As a vet in a busy emergency hospital, I have the utmost appreciation for our team’s incredible hard work and the compassion they show – not just for our patients, but towards each other.
Special thanks, this month, has to go to the incredible veterinary nurses of this world. The compassionate way they carry themselves in the clinic and all the hard work they do always leaves me feeling inspired.
Thank you
“Optimistic, thorough and empathetic.”
Nurses are optimistic, thorough and empathetic – but, most of all, they are the doting advocates and voices for the pets in our hospital. The love, care and kindness they display every shift is incredibly inspiring and, as vets, we really couldn’t do our job without them.
So, rather than a tip this week, I would like to say thank you to veterinary nurses – thank you for supporting us, supporting owners and, most of all, supporting the pets in our care.
In the spirit of Veterinary Nursing Awareness Month, I decided to ask the nurses from where I work – Animal Emergency Service – about their experiences; what they think about being a veterinary nurse and what keeps them coming back day after day.
VN views
Together, we will discover what they find most challenging, how they overcome these obstacles and what tips they have for nurses around the world to make the most of their nursing careers.
Over the next few posts throughout May, I will compile a collection of useful tips our nurses find important in maintaining good mental health, a gold standard of veterinary nursing and positive client communications. I will discuss useful tips on how best to overcome the physical and emotional challenges seen in so many clinics worldwide.